23 Jan 2024
Mark Lowrie shares his ideas around how to manage patient health, medication and owners’ expectations.
Mark Lowrie
Job Title
Image © Marek / Adobe Stock
Epileptic seizures are one of the most common neurological disorders diagnosed in dogs. They also represent some of the most challenging cases in terms of management for first opinion veterinary practitioners.
In this article, the author tries to give his own personal approach to management of the epileptic dog, beginning with a precise diagnosis, accurate administration of medication and, probably most importantly, the proactive management of a client’s expectations.
Given up to one-third of dogs with epilepsy can become refractory (fail to respond appropriately to adequate dosages of conventional medication), inadequate control, despite a clinician’s best efforts, can really test the veterinarian-client relationship.
Consultations often begin with an owner declaring: “My pet has had a seizure.” This assumption should be challenged. Paroxysmal episodes are difficult to characterise because, by definition, they are episodic with long periods of normality.
The paroxysmal nature of these events combined with the possible presence of prodromal or postictal changes is usually suggestive of a neurological condition and makes many owners assume a seizure. However, with the advent of the smartphone, it is now possible to gain an insight into what the owner has observed.
This development has revolutionised the way we manage dogs and cats with paroxysmal episodes, and although a description may appear diagnostic of an epileptic seizure, the reality is often quite different.
Signs that are useful in distinguishing epileptic seizures from other paroxysmal disorders include the presence of autonomic signs (for example, urination, defecation and salivation), loss of awareness and the presence of abnormal behaviour before or after each event (prodromal or postictal phase, respectively).
Other signs that may help, but are not necessarily diagnostic of an epileptic seizure, include the presence of increased tone, stereotypical episodes (each event looks the same), abrupt onset and termination (except reflex seizures), and a short duration of the episode itself (usually less than a few minutes).
The presence of decreased tone during a paroxysmal episode is strongly suggestive of a non-epileptic seizure disorder and a long duration (for example, 30 minutes to 1 hour or more) would also suggest an epileptic seizure is less likely, particularly when accompanied with no postictal signs.
Epilepsy is a term used to describe a brain disorder characterised by chronic, recurring epileptic seizures. Epileptic seizures are paroxysmal, transient events that occur as a result of abnormal neuronal activity in the brain and are manifest by alterations in motor, autonomic or behavioural features.
Multiple causes of epilepsy exist, including brain tumours, inflammatory brain disease and degenerative disorders. Epilepsy affects up to 0.75% of the canine population. The most common type of epilepsy is idiopathic – or primary – epilepsy (IE). In IE, the underlying cause of recurrent seizures is unknown and no identifiable brain disease can be found. Certain breeds are predisposed to IE, which, based on epidemiologic studies, is thought to have a genetic basis.
Seizures may involve both cerebral hemispheres simultaneously (generalised seizures) or affect a more discrete area within one cerebral hemisphere (focal seizures). Focal seizures may progress to become generalised. Most IE patients display generalised tonic-clonic seizures.
During the tonic phase, the patient loses consciousness and falls to one side in opisthotonus with every limb rigid and extended. The clonic phase that follows consists of limb paddling/jerking and chewing movements.
Most IE patients have their first seizure between six months and six years of age, but patients can be older or younger at onset and so this condition is always possible in any age dog. In one study, 75% of dogs with recurrent seizures at less than one year of age (juvenile epilepsy) had no identifiable brain disease. Another study found no apparent cause for seizures in 35% of dogs with seizure onset at more than five years of age (late-onset epilepsy; Arrol, 2012).
IE is diagnosed by ruling out all other possible causes of seizures by having a normal neurological examination, normal blood tests, a normal brain MRI and normal spinal fluid analysis.
It is recommended to initiate the diagnostic process with routine blood tests to investigate potential metabolic (extracranial) causes. Optimal results are obtained when the dog has fasted for 12 hours prior to blood sampling. In situations where this isn’t feasible, scheduling blood sampling for the following day may be a viable alternative. Some of the following tests are particularly important and should be considered:

The question of whether a problem in the brain exists can be answered by questioning the owner carefully about behaviours at home and performing a targeted neurological examination.
A lot of useful information is obtained by questioning the owner on unusual behaviour while observing the patient in the consultation room.
Seizures suggest forebrain disease and clinical signs of forebrain disease include an altered mentation, central blindness, relentless pacing/circling, head pressing and loss of learned behaviour (for example, toileting in the house having previously learned to go outside).
Careful questioning of the owner will answer whether any of these symptoms are present in between the seizures (interictal period). Observation of the gait during history taking may also detect abnormalities that the owner has not noticed.
Neurological deficits should be consistent with forebrain dysfunction and may include mentation changes, central blindness (a decreased to absent menace response with an intact pupillary light reflex) and general proprioceptive ataxia (appearing to have a drunken gait).
Note that all of these signs can be seen in the postictal period (usually for up to 24 to 48 hours), although they would then tend to be symmetrical in nature. Therefore, repeating the neurological examination at least 48 hours after a seizure is recommended whenever possible.
If any abnormalities are detected then advanced imaging of the brain is advised.
Additionally, a normal neurological examination does not infer a normal brain and so advanced imaging should always be considered in a refractory epileptic patient.
Management of epilepsy can present a variety of challenges – not least as often no definitive answer exists as to when to start treatment with anti-epileptic drugs (AEDs). This is partly due to a lack of evidence-based data, but also differing requirements between individual cases including the owner’s ability to medicate the dog multiple times a day, willingness to undertake regular monitoring and comfort with the prospect of unwanted adverse effects.
For the majority of cases, therapy should be initiated if one or more of the following circumstances apply:
Prior to starting medical management, it’s crucial to discuss and manage client expectations. The primary goal of therapy is to reduce the frequency, intensity and severity of seizures with manageable side effects. It’s important to convey that seizure eradication is unlikely and therapy will probably be lifelong. Encouraging clients to keep a seizure diary helps assess treatment response and improve compliance.
When these medications are assessed in clinical trials, successful treatment is often considered to be a reduction in seizure frequency of at least 50%. It is important to consider what this figure would mean to an individual dog’s seizure pattern before commencing therapy. The client must also be aware that therapy is likely to be lifelong and may require regular adjustment, which can present a considerable financial burden.
Encouraging the client to keep a regular seizure diary is extremely useful to evaluate response to therapy and help guide future decision-making. It is also likely to increase compliance, ensuring that AEDs are given at the correct time and dosage.
Effective communication from the initial consultation is vital. Guiding owners towards resources to understand and navigate the care required for an epileptic dog positively influences owner quality of life. Owners should be well-informed and empowered to be active caretakers of their pets. Informed decisions and effective veterinarian-client communication can make a world of difference.
Historically, the focus with IE has been on diagnosing and treating the condition, but increasingly, a recognition exists of the profound impact on the lives of dog owners.
When we consider the quality of life of pet owners, we often refer to the World Health Organization’s definition of health as “a state of complete physical, mental and social well-being, and not merely the absence of disease and infirmity”. It’s a pertinent perspective when we think about how caring for a chronically ill pet can affect our lives. The management of long-term conditions can be challenging and emotionally taxing, similar to the experiences of caregivers in human medicine.
Owners of dogs with idiopathic epilepsy often bear a significant burden. Witnessing their pets’ seizures, managing medication side effects and dealing with the postictal period can be emotionally distressing. Furthermore, the success of seizure control doesn’t always align with the owner’s commitment, leading to feelings of helplessness.
While previous research primarily relied on surveys to understand the impact of canine epilepsy on an owner’s quality of life, recent work by Pergrande et al (2020) takes a more profound approach. It conducts semi-structured interviews, aiming to gain a deeper insight into the emotional and social effects of caring for dogs with IE. Their study revealed the numerous challenges faced by these owners.
The emotional and financial burdens, time constraints, lack of sleep and social isolation all take a toll on their quality of life. The emotional impact is especially significant, often exceeding expectations, and it is even more pronounced when the dog’s seizures are poorly controlled.
What becomes evident is that the emotional bond between dogs and their owners is a powerful force. It motivates owners to pursue treatments and provide the best care for their pets. This bond can be further intensified when dogs exhibit neurobehavioural comorbidities such as increased fear and anxiety – signs commonly seen with IE. Owners of such dogs tend to perceive their relationship as even closer.
The emotional impacts experienced by owners of dogs with IE suggest a need for increased support. Veterinary professionals might need to provide more information about potential challenges and outcomes, even if these discussions are difficult. The use of online resources such as support groups, however, should be viewed as a double-edged sword. While they offer emotional support, they can also overwhelm with perceived negativity.
The current approved choices for monotherapy in treating epilepsy in dogs involve phenobarbital (such as Soliphen), imepitoin and potassium bromide. The selection of an AED is contingent on various factors specific to each case. The ACVIM triangle serves as a valuable guide by assigning an order to prescribe each medication, relying on evidence derived from both clinical trials and clinical experience (Figure 1).
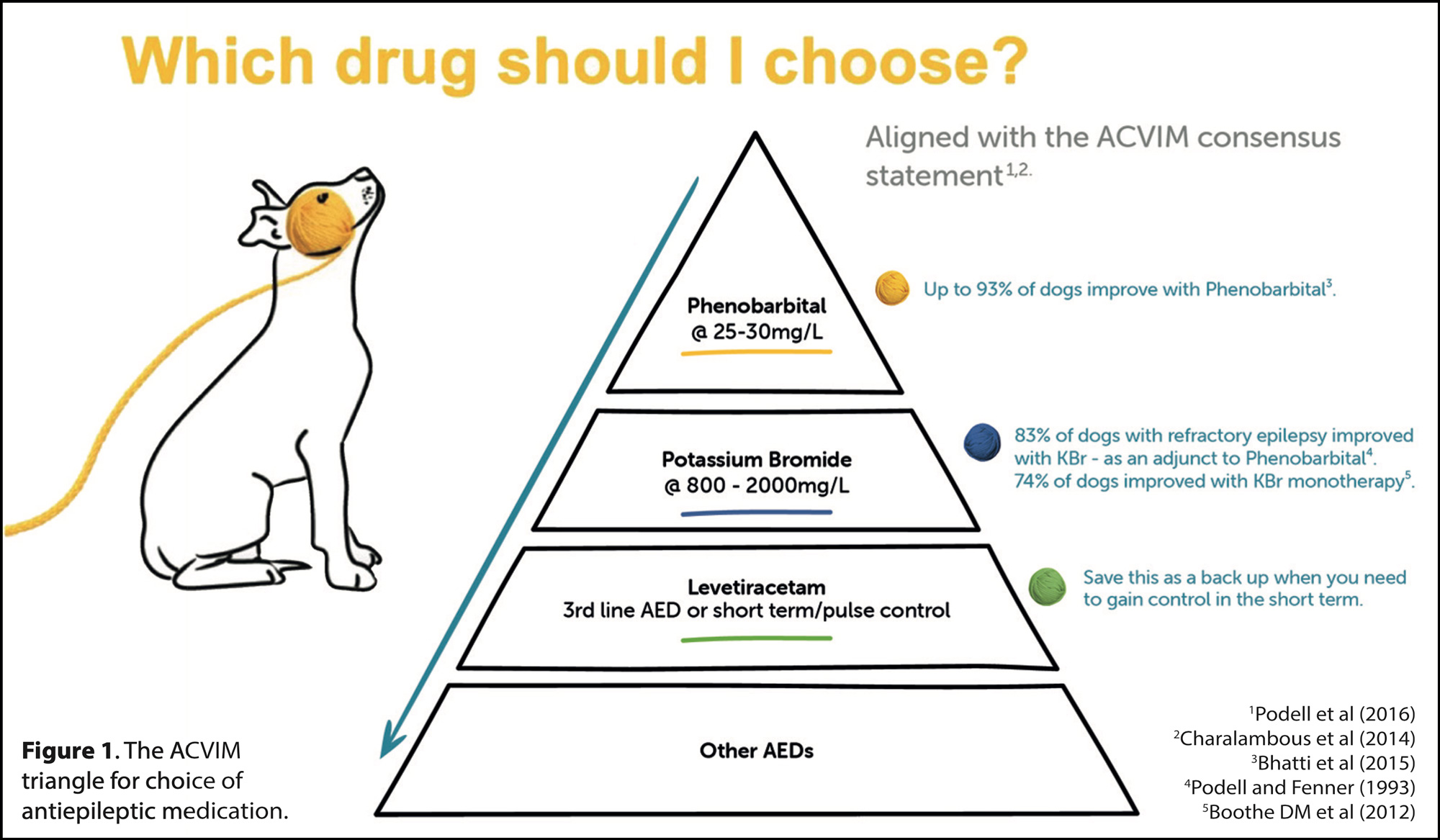
Both phenobarbital and imepitoin are highly endorsed and deemed effective, making them the primary considerations for most epilepsy patients, placing them at the top of the triangle. Imepitoin is indicated for generalised seizures stemming from idiopathic epilepsy, while phenobarbital is licensed more broadly for epilepsy in dogs, making it suitable for managing both structural epilepsy and IE. Phenobarbital is also recognised as effective for treating severe seizures, cluster seizures and status epilepticus, whereas imepitoin is not recommended as a primary treatment for cluster seizures or status epilepticus.
A more recent study (Stabile et al, 2019) examined dogs receiving either imepitoin (n=31) or phenobarbital (n=30) as monotherapy for epilepsy. The study revealed that 67.7% of dogs on imepitoin developed cluster seizures, compared to 36.7% in the phenobarbital group. Additionally, more than 90% of the imepitoin group developed cluster seizures over the three-year follow-up, contrasting with 36.7% in the phenobarbital group.
23% of dogs on imepitoin experienced adverse events necessitating a switch to another medication. These results suggest that, when used as first-line treatment, imepitoin may lead to more frequent and earlier cluster seizures, along with adverse effects, compared to phenobarbital monotherapy. Considering the author’s own clinical experience and these findings, he leans towards recommending phenobarbital over imepitoin as the initial medication for dogs with epilepsy.
Both phenobarbital and imepitoin are contraindicated in cases of severe hepatic insufficiency. Consequently, potassium bromide, which is free of liver metabolism, emerges as a viable option for patients with hepatic insufficiency.
The ACVIM panel awarded potassium bromide a second tier status in the triangle (moderate recommendation and most likely to be effective). A study indicated that 74% of dogs experienced a 50% or greater reduction in seizure frequency with potassium bromide monotherapy (Boothe, 2012).
In instances of serious renal insufficiency, all three options are contraindicated, and the decision to use should hinge on a risk-benefit analysis conducted by the attending veterinarian on a case-by-case basis.
Levetiracetam received a low recommendation from the ACVIM panel and sits on tier three of the triangle. All other AEDs are on the lower level of the triangle as they have little evidence to support their use. None of these drugs are licensed for treating canine epilepsy.
Several reasons exist as to why phenobarbital may not be sufficient in managing epilepsy. Sometimes this may be because the dog has an identifiable underlying cause for the seizures that has not been diagnosed, the dog may be one of the 25% with refractory epilepsy or it may be that the medication is not being administered at the correct dose. However, owner expectation is probably the most common reason for a perceived failure in management of epileptic dogs (Pergrande et al, 2020).
Some patients will require polytherapy to optimally manage their epilepsy, with 20% to 40% of dogs reported to be refractory to monotherapy with phenobarbital. In these cases, adjunct treatment with an additional antiepileptic medication is required.
Potassium bromide has the best level of evidence based on the ACVIM panel recommendations for adjunct therapy and is the only licensed medication for this indication in dogs.
Phenobarbital has a relatively low level of evidence for adjunct therapy. Given that the majority of dogs requiring a second line antiepileptic medication will be receiving phenobarbital as a first line option, potassium bromide is an optimal choice for adjunct therapy – particularly as it works synergistically with phenobarbital. Levetiracetam and zonisamide are also considered in adjunct therapy, but neither of these drugs is licensed for use in dogs.
This article emphasises the critical need for enhanced support, resources, and improved communication platforms to alleviate the emotional and lifestyle challenges experienced by owners of dogs with IE. These insights can potentially enhance the overall caregiving experience for these dedicated dog owners. Initiatives such as the Synaptic Tails podcast, produced in collaboration with TVM and Movement Referrals: Independent Veterinary Specialists, aim to address these issues and develop resources to assist these owners.
Good communication from that first consultation is vital. Signposting resources that can help an owner understand and navigate the care required for an epileptic dog has been shown to positively influence an owner’s quality of life. Failure is often perceived rather than a reality.
A well-informed and empowered owner will serve as an active caretaker of their pet and this can all be achieved through effective veterinarian-client communication.