2 Dec 2019
Panagiotis Kokkinos, Diana Ferreira and Daniela Murgia detail the clinical signs of this issue, and treatment and management options.

Figure 1. Screw tail in a bulldog. The deviation of the terminal coccygeal vertebrae and tail deformation result in tail skin folds. Image: AHT.
Screw tail is an anatomical deviation of the terminal coccygeal vertebrae commonly seen in brachycephalic breeds, resulting in tail fold pyoderma and pain.
Initial medical treatment is usually undertaken, but relapses are common due to the abnormal anatomical conformation. In these cases, surgical treatment is sought.
Surgical intervention – aiming to completely resect the coccygeal vertebrae and associated skin fold – will result in definitive resolution of clinical signs and discomfort, with occasionally mild complications in the short term.
Screw tail, corkscrew or ingrown tail is a condition characterised by ankylosis of the terminal coccygeal vertebrae and tail deformation, resulting in tail skin folds.
In severe cases, the tail is deviated in the ventrocranial direction – consequently causing pressure and friction trauma, and secondary inflammation and infection.
The condition is most commonly seen in brachycephalic breeds, such as bulldogs, French bulldogs, Boston terriers and pugs.
Only a few epidemiological data have been published concerning tail malformation, or tail folds, in brachycephalic breeds. A survey by The Bulldog Breed Council found 75% of exhibited bulldogs had a screw tail (The Bulldog Breed Council, 2016), while a demographic study about the French bulldog population in the UK revealed skin fold dermatitis to be in the top five conditions vets in primary care come across (O’Neill et al, 2018).
Screw tail often creates redundant and deep skin folds around the base of the tail (Figure 1).

The skin-to-skin contact leads to cutaneous inflammation (skin fold dermatitis or intertrigo) as the two opposing surfaces rub against each other, causing localised friction and abrasion.
Tail fold dermatitis is commonly exacerbated by excessive accumulation of debris and secretions, which – along with the coexisting warm and poorly ventilated micro-environment – causes maceration of the skin and secondary bacteria or yeast overgrowth.
Especially in the case of tail fold intertrigo, the risk of contamination of the diseased skin with faecal material always exists due to the proximity to the anus. Additionally, the condition can be exacerbated in obese dogs as the SC fat result in more prominent folds.
Initially, intertrigo lesions are characterised by erythema, exudation and a malodorous scent. With the progress of the condition, pain, pruritus, rubbing and scooting are some common clinical manifestations.
In more severe, complicated cases, the condition progresses to deep pyoderma and ulcers, and sinus tracts may be seen along with foul odour.
During anamnesis, owners may mention their pet does not like to be touched around the region of the tail, or appears in discomfort when trying to sit and changes position frequently.

Behavioural changes – such as excessive licking or rubbing of the perineum, or tail chasing – denote the presence of pruritus due to the established dermatitis; such a behaviour resulting in self-trauma can exacerbate the condition, consequently causing a vicious cycle.
Obtaining a good medical history and performing a thorough physical examination are of great importance.
This will help the clinician to establish the severity of the problem, and identify comorbidities such as obesity, brachycephalic obstructive airway syndrome, gastrointestinal tract diseases and neurological diseases – all of which may affect the patient’s general health.
Concomitant allergic skin diseases or endocrinopathies can exacerbate the clinical signs and complicate treatment.
In patients with clinical evidence of skin fold dermatitis, cytology of the affected area is recommended. Tape strips, impression smears or cotton-tipped swabs can be used to collect samples for examination and help select the appropriate treatment plan.
Deeper skin scrapes or hair plucks (since the area is difficult to scrape) would be required to rule out demodicosis – a condition some brachycephalic breeds can be predisposed to. Deep sedation or general anaesthesia may be required to facilitate complete examination of the affected area and sample collection.
Based on the results of clinical examination and cytology, culture and sensitivity testing may be indicated to guide systemic antimicrobial therapy. Common microorganisms isolated from tail fold pyoderma include coagulase-positive staphylococci, Staphylococcus intermedius, Streptococcus species, Escherichia coli, Pseudomonas species, Proteus species, and yeast such as Malassezia and Candida.

Impairment of the patient’s immune response, concomitant disease, pruritus, scar tissue formation and unwarranted initial therapy are all negative prognostic factors that make the disease more difficult to manage.
Radiographs of the caudal vertebrae will indicate the level and severity of the vertebral ankyloses, and can aid in the surgical planning in some cases (Figure 2). In patients with concomitant neurological deficits, advance imaging (MRI or CT) may be indicated.
Conditions such as perianal fistula, anal sacculitis, perianal tumours, trauma and foreign bodies should be considered possible differential diagnoses.
In many cases where an underlying disease has been identified and successfully managed, medical therapy alone can maintain the condition under control. However, when marked anatomical defects exist – such as severe corkscrew tail – surgical intervention is often required.
Although it will not alter the anatomical conformation of the tail – and, therefore, the main predisposing factor – medical management can be successful, especially in the short term.
Medical treatment is aimed at controlling the associated skin disease by improving the microclimate between the skin folds and balancing the local microflora population, which implicates potentially lifelong commitment. This can be achieved by regular cleaning of the skin folds, the use of topical therapy and parenteral antimicrobials when deep infection is established. However, a desirable outcome requires owner compliance.
Additionally, once an underlying predisposing condition has been recognised, appropriate management of it should be sought, along with the treatment of the tail fold dermatitis.

Topical therapy should be selected on the basis of cytological examination findings, whereas systemic antibiotics should be prescribed after topical therapy alone has failed or deep bacterial infection is present.
Bacterial culture and sensitivity testing are not always necessary; however, they should be performed when lesions are consistent with a deep pyoderma, when rod-shaped bacteria are found on cytology or when empirical antibiotic treatment failed to resolve the infection.
In the case of deep pyoderma, obtaining specimens of the deep tissue via biopsy is preferable to obtain more reliable results.
To facilitate the best penetration of topical medication, the area should be gently clipped to remove soiled hair. The use of antiseptic wipes, sprays, mousses and shampoos may all be used to great effect; products containing chlorhexidine are particularly useful.
Concentrations of chlorhexidine between 2% and 4% provide the best broad-spectrum cover against Gram-positive and Gram-negative bacteria. Shampoos, sprays and wipes provide better cleansing where exudation is present. Acetic acid-based products are useful when Pseudomonas has been isolated.
Other antiseptics that can be addressed in the topical treatment include benzoyl peroxide, chloroxylenol and ethyl lactate. Chlorhexidine preparations with or without antifungal agents can be used in areas where yeast is found.
After antiseptics are used to clean the diseased area, creams or ointments can be applied to the skin folds for protection. Gels do not tend to be as effective, as they are rapidly absorbed and provide no barrier to prevent further skin-to-skin rubbing. Creams and ointments tend to be much greasier and persistent on the skin, and provide better protection. Additionally to the topical protection, creams and ointments containing active ingredients may also be used.
Human products containing antifungal agents (miconazole or clotrimazole) may be used off-licence to treat yeast overgrowth, or products containing fusidic acid or silver sulfadiazine may be used where bacterial involvement is identified.
Once bacterial or yeast overgrowth/infection has been successfully treated, maintenance therapy should be possible using an antiseptic product followed by some form of barrier cream/ointment used once or twice weekly.
Where excessive skin folds are found in obese animals, dietary management to reduce bodyweight can help to adjunctively alleviate clinical signs.
Medical treatment of tail fold pyoderma is often palliative. Often, refractory cases or recurrence can be seen and are highly likely because infection in these cases is secondary to an anatomical deformity of the tail. In these cases, surgical correction is indicated.
Surgery is aimed at removing the redundant skin that forms folds, and caudectomy. An important part of presurgical planning is determining whether tail deviation is part of the problem. If it is, tail amputation is a necessary step to obtain satisfactory results.
In preparation for surgery, a week of medical treatment is recommended to decrease the bacterial burden and the amount of skin inflammation. According to Knight et al (2013), infection rates before surgery account for 41% of the dogs.
Most dogs with tail fold pyoderma and screw tail need a caudectomy to resolve the dermatitis – especially in the presence of a generalised skin disease.
Surgical preparation includes hair clipping of the perineal area, tail base and tail folds. A purse string suture is placed around the anus (Figures 3 and 4).

The dog is positioned in sternal recumbency, with the hindlimbs hanging down the end of the surgical table. This should be well padded to reduce pressure injury to the femoral nerves.
Samples for bacterial culture/sensitivity should be taken before closure of the surgical site, while antimicrobials should be continued postsurgery until the bacteriology results become available.
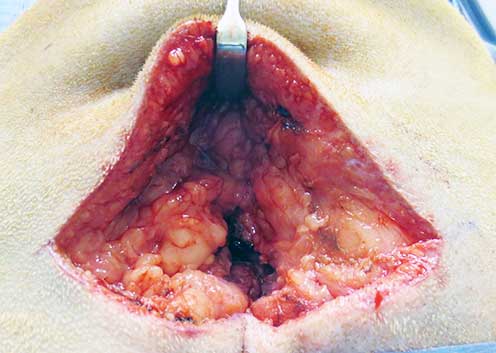
A horizontal elliptical skin incision is made around the entire tail base, preserving the dorsal tail base skin to provide a more cosmetic outcome (Figure 5). Care must be taken to the depth of dissection ventral to coccygeal vertebrae, because perineal diaphragm structures and the rectum are immediately ventral to the tail base.
Once the caudectomy is performed, a decision is made whether an active drain needs to be placed. In general, if postsurgical dead space is limited, placement of a drain is not required (Figure 6).
During closure, care must be taken so that large deep bites are avoided, because the rectum and neurovascular structures – such as the perineal and caudal rectal nerves, as well as the pudendal nerves and arteries – could be penetrated or entrapped.
The remaining tail base skin is trimmed to include any excess tail fold present, and the area closed routinely (Figures 7 and 8).
Scant published data exists regarding postoperative complications of caudectomy.

In two studies, only mild, short-term postoperative complications were seen (Knight et al, 2013; Abrescia et al, 2017). The complications included abscess formation in 27% of the dogs (Abrescia et al, 2017), while decreased rectal sensation with adequate anal tone, failure to posture to defecate, and postoperative draining tracts were reported in 12% of dogs immediately after surgery (Knight et al, 2013).
In the latter study, delayed wound healing and wound inflammation, persistent tail chasing behaviour and temporary changes in defecation habits were described in 13% of dogs soon after surgery (Knight et al, 2013).
Nevertheless, both studies reported good to excellent long-term outcomes in brachycephalic patients with screw tail following caudectomy, while Simons et al (2014) reported similarly high levels of owner satisfaction.
Caudectomy provides good to excellent long-term outcome in dogs with screw tail and related tail fold pyoderma where cases failed to respond to medical management.
The procedure can be challenging to perform, so good presurgical planning must be considered. Owners should be aware of the potential postoperative complications, and that the surgical approach provides a definitive treatment aiming to alleviate the dog from discomfort and pain, and absolve themselves from the long-term commitment medical management requires.