5 Sept 2016
Sally Birch discusses the case of Simon, a four-year-old male, neutered domestic shorthair cat, after he was rushed to surgery having been hit by a car, in the latest Case Notes series.
Sally Birch
Job Title
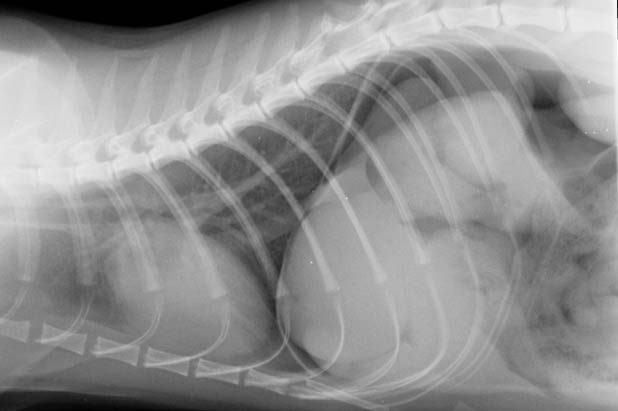
Figure 1. Left lateral radiograph of the caudal abdomen and pelvis.
Simon is a four-year-old male, neutered domestic shorthair cat. He has been rushed to your surgery by his owner, having been hit by a car.
He is recumbent and, on examination, shows signs of caudal abdominal pain.
You stabilise him with analgesia and intravenous fluid therapy, before acquiring survey radiographs of the thorax and abdomen/pelvis to assess for injury (Figures 1 and 2). Orthogonal views were also acquired.
What are the key radiographic and ultrasonographic findings?

In Figure 1, the descending colon is mostly gas-filled in the mid-abdomen.
Unusually, the serosal surface of the colonic wall is visible, indicating the presence of free peritoneal gas (that is, pneumoperitoneum). This is further supported by the gas lucency, which surrounds the right kidney and highlights the sublumbar muscles. Further evidence of pneumoperitoneum is present in Figure 2.
Free gas typically collects at the highest point in the abdomen and, when an animal is in lateral recumbency, gas tends to collect in the craniodorsal abdomen, adjacent to the diaphragm and liver lobes. It is not normally possible to see the peritoneal surface of the diaphragm, since being soft tissue in opacity, it would normally be expected to border efface with the soft tissue opacity of the liver. Here, gas is present on both sides of the diaphragm (that is, in the lungs and in the peritoneum) and, therefore, the diaphragm is visible as a discrete and separate linear structure dividing the thoracic and abdominal cavities.
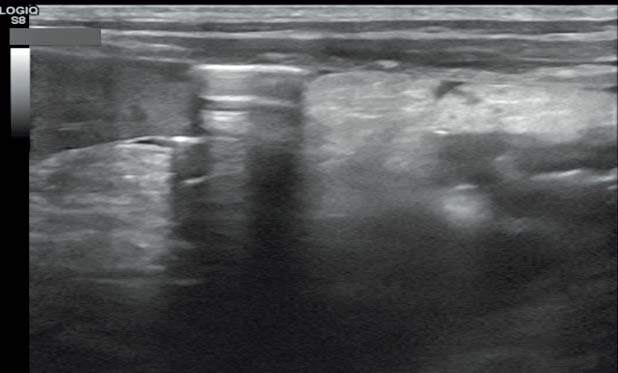
On the ultrasound image in Figure 3, a discrete hyperechoic line just ventral to the abdominal wall is present, which is not located within a loop of intestine and is associated with reverberation artifact, distally. This is the typical appearance of free peritoneal gas. It is important not to mistake gas within the lumen of the thin-walled colon or gas within the lung when imaging the cranial abdomen as free gas. The most common causes of pneumoperitoneum include recent abdominal surgery or abdominocentesis and gastrointestinal tract rupture.
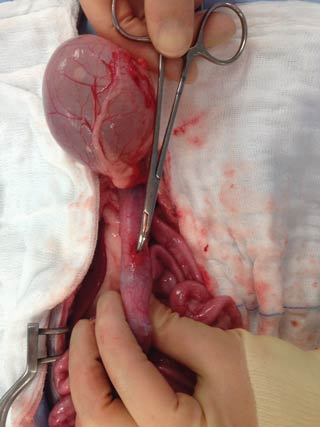
In Simon’s case, a fragment of pubic bone had perforated the colonic wall, resulting in septic peritonitis (Figure 4). A less common cause of pneumoperitoneum is perforation of the abdominal wall, usually as a result of trauma. Ultrasound is more sensitive than radiography for the detection of small volumes of free gas.
Acquiring a ventrodorsal view of the cranial abdomen of an animal in left lateral recumbency, with the cranial abdomen elevated using a horizontal beam, increases the chances of detecting small volumes of free peritoneal gas using radiography (appropriate radiation safety measures should be observed).
Simon made a full recovery following exploratory abdominal surgery to repair a hole in his colon.