24 Feb 2021
Will Robinson BVetMed, MSc, BSAVA PGCertSAS, DipECVS describes how to perform both these procedures in dogs and any potential complications that may occur after.
Will Robinson
Job Title
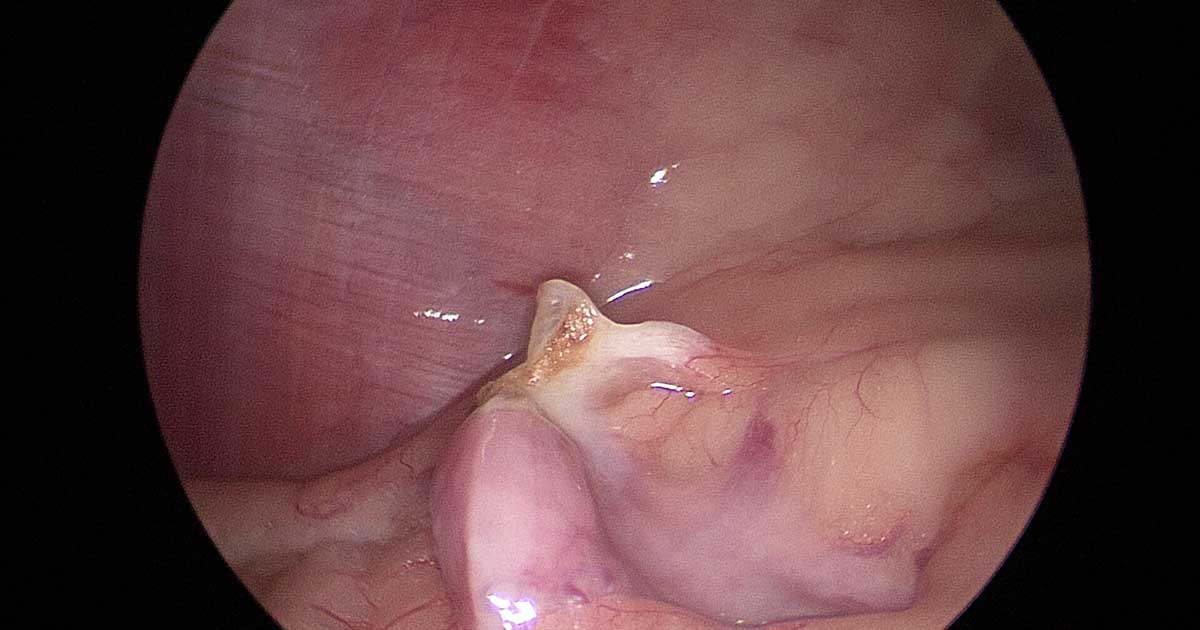
Figure 5. Inspection of the pedicle after the ovary has been removed.
The term spay is often used to describe the process of gonadectomy in female dogs and cats.
In the case of a bitch, this specifically would equate to an ovariectomy (OVE). However, it is often used synonymously with ovariohysterectomy (OVH), despite this procedure involving removal of the uterus as well as the ovaries.
Elective sterilisation is by the far the most common reason for performing an OVE or OVH in companion animals. Other reasons for performing these surgeries include treatment of ovarian and uterine diseases such as neoplasia, pyometra, uterine torsion or rupture.

The choice of which procedure is performed is largely based on geographical location and the teaching practice of the institute where the individual veterinary surgeon trained. When these procedures are performed for reasons other than elective sterilisation, the choice of technique can be dictated by the presence or absence of uterine disease.
Surgery is commonly performed “open” via a celiotomy, but has also been reported using various laparoscopic techniques, which are growing in popularity.
Multiple studies have failed to show a difference in outcome or complications when considering OVE versus OVH. The benefits of laparoscopy include decreased pain, less risk of catastrophic wound dehiscence and shortened hospitalisation time1. These benefits have not been demonstrated when considering laparoscopic methods versus open procedures in cats.
Commonly reported advantages for performing sterilisation are:
Two systematic reviews in dogs demonstrated that insufficient evidence existed to conclude that timing of neutering is related to the risk of development of urinary incontinence or mammary neoplasia2,3.
Many variations of OVH exist, but the overall technique remains the same. No studies to date have reported an advantage of one variation over the other.
The ventral abdomen is clipped from 2cm to 4cm cranial to the xiphoid process of the sternum to 2cm to 4cm caudal to the cranial pubic brim. Laterally, the clip extends lateral to the nipples. The area is prepared aseptically.
An incision is made just caudal to the umbilicus. Short incisions have been linked to ovarian remnant syndrome and should be avoided when the procedure is performed by inexperienced surgeons.
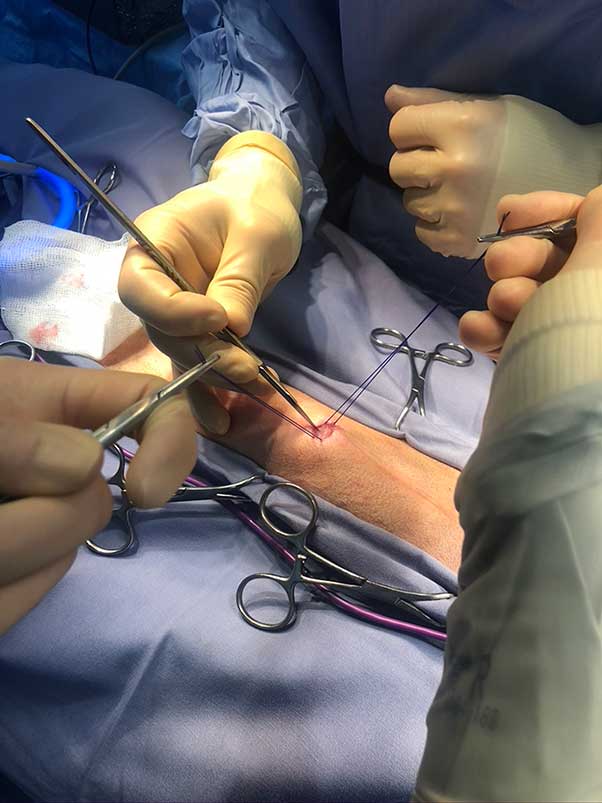
An incision is made through the skin, SC tissue and then a stab incision is performed through the linea alba. The incision in the linea alba can then be extended with sharp dissection with scissors.
The first ovary can be located with a spay hook or using the surgeon’s fingers. The suspensory ligament should be disrupted and the author routinely achieves this by using gentle pressure while grasping the ovary.
Some surgeons will transect the ligament with sharp dissection and others may use electrosurgery. This may not be required in all dogs or cats if adequate exposure of the ovary and associated vessels exists.
A window is then made in the mesometrium, in an area with minimal fat and away from the ovarian vessels. The ovarian vessels should then be ligated with absorbable sutures, such as polydioxanone or polyglactin 910. Non-absorbable sutures and cable ties have been associated with chronic sinus formation, and should be avoided where possible.
A three-clamp technique can be performed with the ligatures tied in the crush zone of the proximal clamp. A surgeon’s throw can help maintain adequate knot friction while the remaining throws are placed without the tissue overcoming this and the knot loosening. Other surgeons will use a sliding or a modified millers knot to overcome this issue.
The mesometrium can then be bluntly divided in many animals without the requirement for cautery or ligature placement. However, in animals where the procedure is being performed at the time of oestrus, additional bunch ligatures or electrosurgical haemostasis may be required.
The uterine body and cervix should then be exposed, and a transfixing suture placed around the uterine vessels lateral to the uterine body on either side, followed by a circumferential ligature. Care should be taken not to penetrate the lumen of the cervix or uterus when placing the transfixing ligature. The use of clamps should be avoided where possible, as the uterus can be friable.
All vascular pedicles should be inspected for ongoing haemorrhage before closure. The author does not routinely oversew the uterine stump at this stage. The linea alba, SC tissue and skin should be closed routinely.
The procedure for performing an OVE is very similar to the initial steps previously described for an OVH. Once the ovarian vessels have been ligated, the proper ligament is located just caudal to the ovary and the uterine vessels are ligated at this level.
If the uterus appears abnormal an OVH should be performed. The proper ligament should then be transected at the level of the tip of the uterine horn. The abdomen is then closed routinely after inspection of both pedicles for evidence of haemorrhage.
Laparoscopic OVH and OVE have been described and no significant evidence exists that one technique is superior than the other. In the author’s institution, an OVE is performed via a three-port technique, which will be described. Single and two-port techniques are also reported, with the latter being associated with reduced surgical operating times when compared with the former.

The patient is prepared in a similar fashion to an open procedure and the clipped area remains relatively narrow. The animal can be placed in a 15° Trendelenburg position by elevating the caudal half of the dog to improve visualisation of the ovary and uterus, but in the author’s experience this is rarely required.
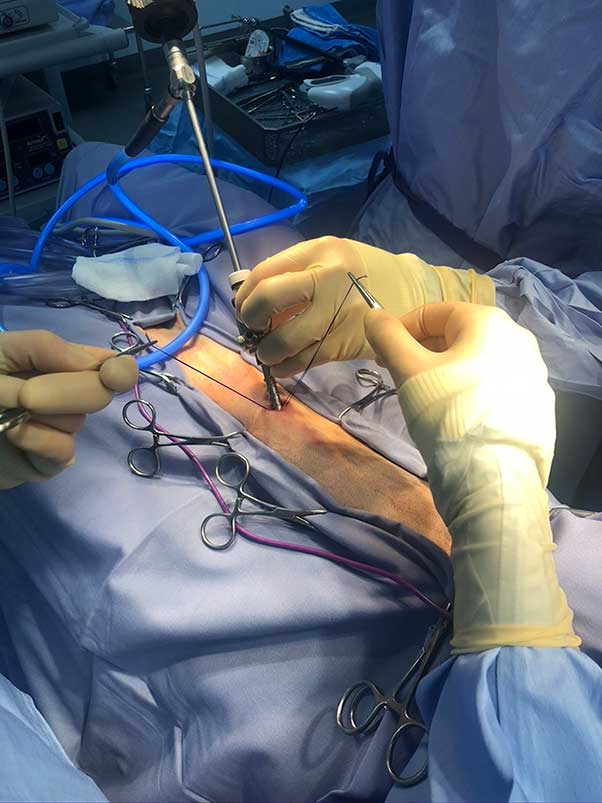
The theatre setup used at the author’s institute is shown in Figure 1. A pneumoperitoneum is normally established via a modified Hassan approach or with a Veress needle using CO2. The author aims to maintain abdominal pressure around 8mmHg to 10mmHg, which often allows adequate visualisation without significant depression of ventilation or cardiovascular parameters.
The first cannula is inserted 3cm caudal to the umbilicus on the midline, through which the laparoscope is inserted (Figure 2). Two more instrument ports are placed approximately 3cm to 5cm cranial and caudal to the first port. This allows placement of a probe or laparoscopic Allis tissue forceps alongside a bipolar vessel sealing device. The patient can now be tilted to one side to visualise the first ovary.
The ovary should be grasped at the level of the ovarian bursa (Figure 3) and the vessel sealing device used to cauterise the ovarian vessels and transect through the proper ligament (Figure 4). The pedicle is visualised for 60 seconds before the ovary is removed to check for any evidence of haemorrhage (Figure 5).

The ovary is removed via one of the portals. In larger dogs, a 10cm port is often used in preference to a 5mm port caudally to facilitate this removal. It is important to check the entire ovary is present in the excised tissue to eliminate the risk of the dog developing ovarian remnant syndrome in the future.
The process is repeated on the other side. Once the procedure has been completed the abdomen is deflated, and sutures are placed in the linea alba, SC tissue and skin.
The most common complication reported after OVH is haemorrhage, which is more common in dogs weighing more than 25kg. This is also reported as the most common cause of death after an OVH.
Obesity and a small incision appear to be risk factors for this complication in dogs undergoing an OVH, with the right ovarian stump being the most likely side that will be affected. This is commonly recognised at surgery, but some dogs can develop this in the immediate postoperative period and show signs associated with hypovolaemic shock. The incision should be extended if this is encountered at open surgery or converted to an open procedure if being performed laparoscopically.
The pedicle is visualised using the colonic manoeuvre to access the left ovarian pedicle and the duodenal manoeuvre for access to the right prior to additional ligature placement. The pedicles should normally be located at the caudal pole of each kidney.
Conservative management using body bandages can be used in dogs postoperatively, alongside appropriate fluid therapy, but taking the animal back to theatre may be required if this is not successful.
Another important complication is ovarian remnant syndrome, resulting from incomplete excision of ovarian tissue. To reduce this occurring, the author routinely checks the tissue resected at surgery to ensure the ovary appears intact regardless of the surgical procedure performed. Again, the right ovary appears to be more commonly affected than the left side due to its more cranial position reducing the ability to expose it at surgery.
A study by Ball et al4 showed that surgical error was the most likely cause of ovarian remnant syndrome, rather than the presence of true ectopic tissue.
Pyometra is often described as a concern following OVE as the uterus is not removed. Two studies did not find any dogs that had an OVE that then developed a pyometra postoperatively, and to the author’s knowledge no other reports of this occurring exist.
One of the studies previously mentioned5 did show that in cases where a stump pyometra developed after OVH, ovarian remnant tissue was also present. This supports the notion that proper surgical technique is important to minimise the risk of development of pyometra or stump pyometra in the future. Exogenous progesterones should also be avoided where possible.
Okkens et al5 also concluded that dogs that have had an OVE are not at an increased risk of developing pyometra when compared with dogs undergoing OVH.
Granulomas are reported after both OVE and OVH, largely when non-absorbable sutures have been used at surgery. This complication has decreased considerably since the introduction of absorbable suture materials.
Injury to the urinary tract can occur during surgery and is often associated with poor exposure. Most commonly the ureters are included accidentally in the ovarian or cervical ligatures. The true incidence of this is unknown due to the potential for unilateral ligation to go undiagnosed in the presence of a healthy contralateral kidney.
Incontinence is often one of the complications that owners have often heard about and is a source of reluctance to spay their animal in the first place. Urethral sphincter mechanism incompetence (USMI) is a complex, multifactorial condition that is considerably more likely to occur in spayed individuals (up to 90% of cases) over entire ones. However, association between the age at the time of spaying and the development of USMI is controversial.
A recent systematic review confirmed that the evidence is not strong or consistent enough to support any recommendations as to the specific effect of timing of spaying the dog and the development of USMI3. While age at the time of surgery is not currently considered a risk factor, this does not detract from the higher incidence of USMI reported in neutered females.