30 May 2016
Ariane Neuber outlines the factors involved in ear inflammation in canines and explains the importance of cytology in choosing the correct antibiotic and cleaning method.
Ariane Neuber
Job Title
Figure 5. Excessive cleaning fluid is gently removed using a swab, cotton wool or tissue.
A dog’s sense of hearing is far more acute than a human’s and is important for how it interacts with its environment.

Otitis is common in dogs and very painful. A study of stray dogs euthanised for aggression found about a third had severe and unrecognised signs of otitis on postmortem, possibly contributing to their aggressive behaviour (Clark, 2005).
The condition tends to relapse – frustrating the patient, owner and attending veterinary surgeon – unless it is managed well. It is one of the most common reasons for a dog to be presented to a veterinary practice and a common reason to change practice if it cannot be satisfactorily controlled.
Cases of otitis occur because an underlying disease creates an environment allowing the proliferation of the microorganisms to a level causing overt clinical signs.
Clinical signs include otic discharge, otic pruritus, head shaking, pain, swelling leading to stenosis and malodour. Most organisms found in otitis cases are a normal part of the bacterial flora in this body region; however, transient organisms are sometimes cultured.

Table 1 provides an overview of the potential underlying diseases (primary factors) and factors that contribute to the development of the disease, but do not lead to clinical disease on their own (predisposing factors; Figures 1 and 2). The disease leads to changes, such as stenosis, scarring hyperplasia of the ceruminous glands and possible calcification/ossification, making future episodes more likely. Therefore, the fact a patient has had otitis once makes it likely to reoccur. These factors are called perpetuating factors.
Many patients with an underlying allergy suffer from low-grade, potentially unrecognised otitis that only becomes an issue when proliferation of the microbial population leads to more severe clinical signs, prompting the owner to seek veterinary advice.
In addition to the aforementioned factors, increased numbers of microorganisms push the patient over the comfort threshold and lead to visible signs of otitis.
Microorganisms commonly seen in otitis are Malassezia yeast and Staphylococcus; however, Streptococcus, Pseudomonas, coliform bacteria, Klebsiella, Proteus and Escherichia coli cases also exist. These infections lead to an acute flare, and must be identified and treated appropriately.
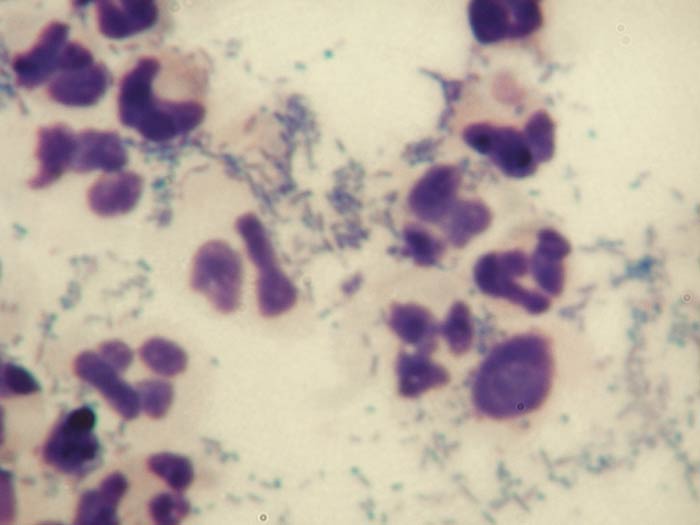
Most cocci have a predictable pattern of antibiotic sensitivity, whereas rods are erratic in their antibiotic resistance. It is, therefore, important to identify whether yeast, cocci or rods are involved in the infection. This will lead to a major difference in the decision for treatment and further tests.
Cytology is important in the decision-making process for otitis cases. When rods are seen on cytology, culture and sensitivity testing is important to make the most suitable antibiotic choice and to be able to give a more precise prognosis (Figure 3).

Cytology is a quick and – with experience – relatively easy and rewarding diagnostic test, which is cost-effective and gives valuable information.
A good microscope is essential for successful cytological examination. Most practices have other equipment to hand, such as glass slides, cover slips, immersion oil, clear sticky tape, needles, syringes, cotton buds and rapid staining solutions – ideally a modified Romanowsky stain.
For otic cytology, a sample is taken with a cotton bud and carefully rolled on to a slide. Different staining techniques exist and the quality of the otic discharge is an important factor in choosing the most suitable method.
Purulent samples may be best air dried, fixed in the fixing solution by dipping the slide 10 times for a second each time, followed by 10 dips in the “red” and “purple” solutions each. The sample is then carefully rinsed with water and either air dried, or dried with a hand dryer or hair dryer.
Oily samples may need to be heat fixed before undergoing the staining sequence. Many dermatologists will apply a drop of purple stain to the area covered in the sample, leave it for about 10 seconds and gently rinse with water before drying the slide. This technique does not give good cell detail, so is unsuitable for tumour cytology.
For inflammatory cytology, when only inflammatory cells and microorganisms are expected, the stain is adequate. Once the sample is dried, a drop of immersion oil is applied, a cover slip is laid on top and the sample is examined under a microscope. Initially, a low magnification is used to get an overview and find a good site to examine closer. An area with a good amount of purple-stained structures lends itself to further examination.
Higher magnification lenses are then chosen, to a magnification that may require immersion oil on top of the cover slip as well. The nature of the cells – for example, keratinocytes, neutrophils, macrophages and eosinophils – and the presence and nature of the microorganisms, such as cocci, rods and yeast – are noted.
The presence of rods in a sample should always prompt a culture and sensitivity test as Pseudomonas aeruginosa could be present. If it is present, aggressive therapy needs to be started early.
The cytological findings also influence the choice of cleaning solution. Neutrophils and pyogranulomatous samples respond better to cleaning with an aqueous solution, while waxy samples with predominantly keratinocytes and organisms, such as yeast, tend to do better using a cleaner containing ceruminolytic agents.
Healthy ears self-clean; this is called epithelial migration. The outward growth of the keratinocytes, from the tympanic membrane to the opening of the ear canal, effectively removes the small amounts of debris. This mechanism fails in otitis, as it is overwhelmed by the large amounts of debris.
Ear cleaning is a vital part of managing otitis externa. A carefully chosen cleaner removes debris that can harbour microorganisms. The cleaner can be antimicrobial, helping restore normal microflora, enhancing antibiotic action and removal of debris, and enabling thorough examination of the deeper structures of the ear canals.
The method – home cleaning versus in-practice cleaning, conscious or under general anaesthetic – depends on the temperament of the patient, the severity of the disease, the ability of the owner to effectively clean the ears at home and the nature of the infection.
Small amounts of earwax can be cleaned at home if the owner is capable and the dog is amenable. Severely painful ears – for example, in cases of Pseudomonas otitis – require in-practice cleaning under general anaesthetic with good analgesia, followed by at-home top-up flushes.
Cleaning is usually combined with eardrops containing antimicrobial and anti-inflammatory agents. Follow-up appointments are vital to ensure success.
Home cleaning is suitable for mild cases and maintenance therapy in mild, long-standing cases of otitis – for example, mild Malassezia otitis due to atopic dermatitis – and to aid the resolution of more severe cases of otitis as part of an overall management programme.
The cleaning solution needs to be chosen carefully. The chosen cleaner is instilled into the opening of the ear canal, flooding it, with the base of the ear massaged and any excess cleaner with debris carefully wiped out (Figures 4 and 5). This process needs repeating until no debris is seen.
Cleaning is predominantly achieved by mechanical removal of the debris and helped by the ceruminolytic or surfactant effect of the cleaner.
Owners often use too little cleaner or only wipe the outside of the ear with the product applied to a tissue, as they are worried about inducing pain. It is important to demonstrate or explain the best method.


Many cases of otitis leave the patient in severe pain (probably comparable to severe toothache), and conscious examination and cleaning are not possible.
Adequate analgesia needs to be administered for the procedure. The patient should be intubated with a tightly fitting or cuffed endotracheal tube to avoid aspiration of cleaning fluid. The clinician and ancillary personnel should protect themselves from contaminated aerosols, especially in cases of multi-resistant Pseudomonas otitis or MRSA/meticillin-resistant Staphylococcus pseudintermedius.
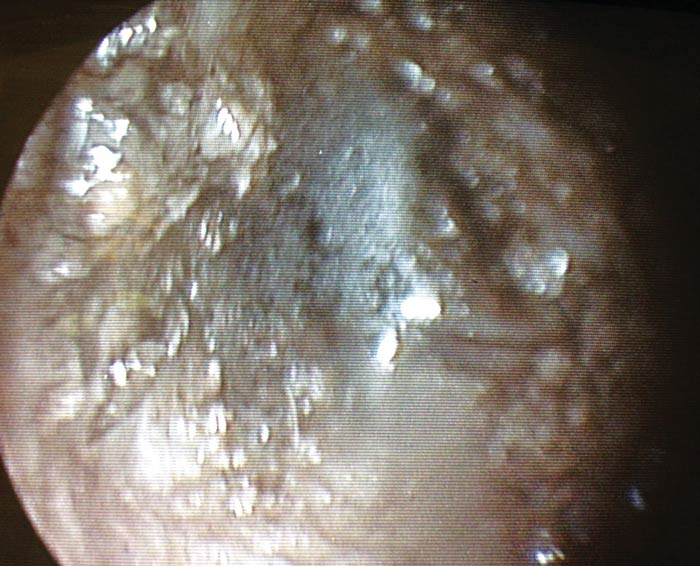
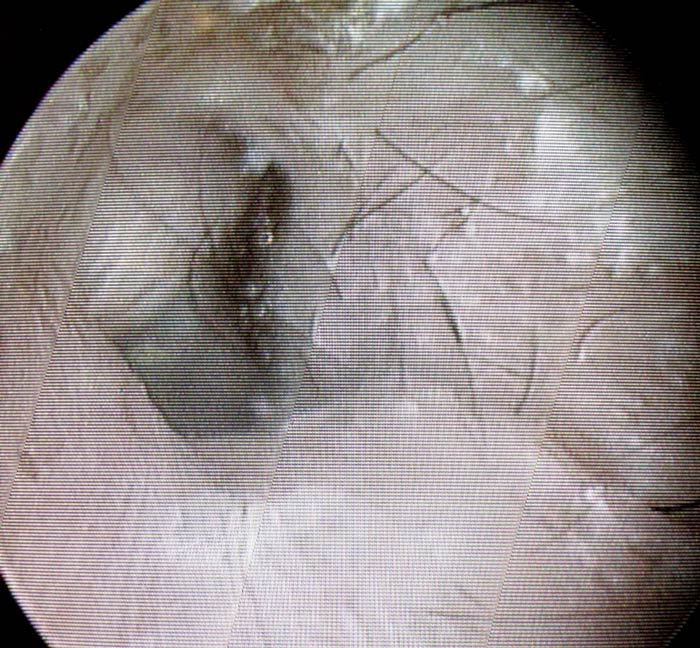
A handheld otoscope can be used, but a videootoscope gives a far superior view, making the cleaning process more thorough and safer for the patient (Figures 6 to 8).
In some cases, when middle ear disease is confirmed or suspected, the tympanic membrane may need artificially rupturing to gain access to the bulla and allow for diagnostics (cytology or culture), visualisation and cleaning of the middle ear cavity.
Due to the presence of nerve fibres in the tympanic cavity, vestibular syndrome, facial nerve paralysis, Horner’s syndrome and deafness are potential problems after an aggressive ear flush. This risk appears low when performed by a skilled clinician.

Numerous ear cleaning products exist and it is worth getting familiarised with the differences. None are suitable in each and any given clinical situation, so multiple products may need to be stocked or ordered on demand.

The choice of cleaner is determined by the nature of the debris and infection. Waxy debris requires the use of a ceruminolytic cleaner (Table 2), whereas purulent discharge responds better to aqueous products containing surfactants.
Ototoxicity is possible if any substance reaches the middle and inner ear. This could be an ear cleaner, drops, inflammatory cells, microorganisms and their by-products or flushing solution, to name a few.
Ototoxicity is uncommon in a clinical situation. It is worth warning the owner of this risk, particularly if in-practice cleaning is carried out and if the integrity of the tympanic membrane is unknown.
Clinicians need to be aware of substances more likely to cause problems and those safe for use in the middle ear. Panel 1 lists a few known ototoxic drugs. Fluoroquinolones, squalene, tromethamine-ethylenediaminetetraacetate (known as TrisEDTA), clotrimazole, miconazole and dexamethasone are deemed to be relatively safe in the middle ear. No ear preparation is licensed for use in case the tympanic membrane is compromised, with only anecdotal evidence to support this.
Ticarcillin, polymyxin B, neomycin, tobramycin and amikacin are potentially ototoxic in dogs with a ruptured tympanic membrane.
Systemic therapy can help in very select cases of otitis.
Systemic preparations – such as selamectin or moxidectin spot-on – are useful in cases of ear mite infestation.
Some cases of otitis media can benefit from systemic antimicrobial therapy; however, topical therapy can reach far higher concentration and should always be tried in amenable cases of otitis externa.
Patients with severe inflammation can benefit from systemic glucocorticoids to provide analgesia and reduce swelling. They also have an otoprotective effect.

After a course of eardrops and regular cleaning, it is important to monitor progress with clinical examination and follow-up cytology. In addition, the underlying primary disease needs to be investigated and managed.
Further tests – such as advanced imaging or allergy testing – may be indicated. A long-term strategy to avoid relapses often includes the regular use of ear cleaners.
Ear cleaning is a vital part of managing otitis externa in dogs. Many products containing a variety of ingredients, and suitable for different clinical situations, are available and it is important for clinicians to familiarise themselves with their properties.
Depending on the cleaner chosen, cleaning removes debris (left in situ, the debris acts like a foreign body and irritates the ear canal), allows for visualisation of the deeper structures of the ear canal, enhances the antibiotic action, is antimicrobial and mechanically reduces the number of organisms.
Ear cleaning is important in the treatment of acute episodes of otitis, as well as in long-term management of chronic cases.