22 May 2020
Francesco Cian DVM, DipECVCP, FRCPath, MRCVS presents the case of a mixed-breed dog referred for the presence of multiple lesions on the tongue, and enlarged submandibular and prescapular lymph nodes.
Francesco Cian
Job Title
Figure 1 (right). The multiple raised lesions on the dog’s tongue. Image: © Fitzpatrick Referrals.
A 12-year-old mixed-breed dog was referred for the presence of multiple lesions on the tongue (Figure 1), and enlarged submandibular and prescapular lymph nodes.
At clinical examination, the tongue lesions measured up to 1cm in diameter, were pink in colour and raised, with distinct borders.
The veterinarian performed fine needle aspirates of both tongue lesions and enlarged lymph nodes, and submitted the slides to an external laboratory for cytological examination.
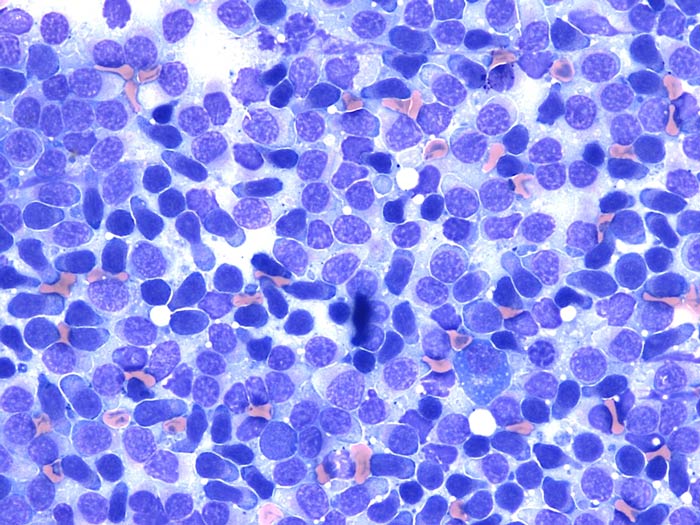
The aspirate from the tongue (Figure 2) was highly cellular and contained a main population of lymphoid cells on a lightly basophilic background. These cells appeared small to intermediate in size and had scant to moderately expanded pale blue cytoplasm, which often formed a small tail, giving the cells a typical “hand mirror” shape.
Nuclei were small to intermediate in size, round in shape, with coarse, nuclear chromatin and occasionally poorly visible nucleoli. Rare mature plasma cells were also noted. Cytological findings in the lymph nodes were similar.
Cytological interpretation was highly suggestive of small cell lymphoma.
Further investigations to confirm the suspicion of lymphoma were recommended. These included flow cytometry, histopathology and/or PCR for antigen receptor rearrangements (PARR) assay. The veterinarian requested PARR testing to avoid a second sedation for collecting a new sample.
A clonal T cell receptor rearrangement was identified, giving further support to the initial diagnosis and confirming small cell lymphoma. In particular, given the size and shape of most cells (small lymphoid cells with hand mirror appearance) and the PARR results (clonal rearrangement of the T cell receptor), a T zone lymphoma (TZL) was considered very likely.
The dog was referred to a specialist oncologist centre. Clinical staging, and liver and spleen cytology were performed.
Both samples harvested an increased number of small lymphoid cells, similar to those observed in the tongue. PARR assay was performed on the splenic aspirate and confirmed the presence of monoclonal population of lymphoid cells.
The patient received lomustine (70mg/m2 by mouth every three weeks; used under the cascade).
Peripheral lymph nodes showed a mild decrease in size, whereas the tongue lesions persisted. At two months from the initial presentation, the disease was stable.
Never completely rule out a differential diagnosis only because it is unlikely – especially if this is supported by some clinical or laboratory data. In those circumstances, consider asking the opinion of an expert and/or perform further investigations to confirm your suspicion.
This case is a good example of a common neoplasm (lymphoma) in a very unusual location (tongue), where other tumour types are more frequently seen.
Neoplasms of the tongue in dogs are rare and account for about 4% of all tumours that involve the oropharynx. The most common tumours found in the tongue are squamous cell carcinoma and melanoma.
Lymphoma in the tongue rarely occurs in dogs and has been recently documented in a case series study in Veterinary Comparative Oncology. All 12 cases were TZL. This is a relatively common subtype of indolent small cell lymphoma, most often involving lymph nodes.
Cytologically, it is characterised by an expansion of main population of hand mirror‑shaped small lymphocytes originating from the paracortical area of lymphoid follicles. These neoplastic cells have a distinctive immunophenotype characterised by loss of expression of the panleukocyte marker cluster of differentiation (CD) 45 and variable expression of other T cell markers (for example, CD3, CD4 and CD8).
Therefore, it is possible to diagnose this form of lymphoma based on cytology and flow cytometry only, and histopathology and immunohistochemistry may not be necessary.
From a clinical point of view, TZL is a slowly progressive and indolent disease. The cases of the aforementioned publication were treated with a variety of therapeutic options – from surgical excision, to multi‑agent chemotherapy, to palliative radiation. All but one achieved complete remission or stable disease. Median survival time was not provided because only two dogs died during the study period; however, 10 of 12 dogs were still alive at publication (27 days to 893 days post‑diagnosis).
Histopathology, PARR and flow cytometry are diagnostic tests often requested to confirm and/or refine a lymphoma diagnosis. Flow cytometry and PARR are less invasive than histopathology, not requiring a solid biopsy to be taken.
Flow cytometry is considered one of the tests of choice to confirm the diagnosis of lymphoma and establish its immunophenotype. However, this technique requires a new, fresh sample to be submitted to a dedicated external laboratory and this should be, ideally, analysed within 24 hours from collection.
PARR assay’s advantage is it can be performed on almost any sample – including pre-stained cytology smears – and, therefore, does not require additional sampling. It is a valid test to confirm or rule out lymphoma when a cytological diagnosis is not possible. However, false negative and, occasionally, false positive results may occur. Therefore, it should not be used as a first line test, but only as a confirmatory one. It is not the preferred test for immunophenotyping purposes. In fact, it may be clonality results are not reflective of a cell’s true immunophenotype. This may be seen in cross-lineage rearrangements of T cell receptors in diffuse large B cell lymphomas or plasma cell neoplasms.