26 Jan 2023
Philip Witte BSc, BVSc, CertAVP(GSAS), DSAS(Orth), MRCVS outlines this condition – typically accompanied by OA – as well as the options available for treating it.
Philip Witte
Job Title
Image: © MilsiArt / Adobe Stock
Elbow dysplasia causes lameness in young dogs and OA in older dogs. Medial compartment disease is one step in the progression of OA, in which OA is reasonably advanced in the medial aspect and not in the lateral aspect of the elbow joint.
While some degree of non-surgical management of elbow OA will be required for all dogs with elbow dysplasia, some surgical options exist for the dysplastic elbow with minimal OA and elbows with medial compartment disease. Aims are to improve comfort in the short term and to minimise the rate of progression of OA in the longer term. This is achieved through restoration of joint loading in the early stages and an attempt to significantly reduce loading through the medial aspect of the joint in medial compartment disease. Salvage includes arthrodesis and elbow replacement, both carrying uncertain prognoses.
A thorough understanding of conservative management is vital, regardless of whether surgical options are pursued at any stage.
Four conditions, often co-existing in a single elbow, have been recognised under the blanket term “elbow dysplasia”.
Elbow dysplasia causes lameness in young dogs and, inevitably, precipitates elbow OA. The four conditions are given in Panel 1.
The rate of progression of OA in elbows affected by elbow dysplasia is unpredictable. Management requires the clinician to have a broad understanding of the wide variety of treatment options in addition to a sensitivity to the needs of the client and the patient.
This article aims to focus on the adult dog with clinically relevant elbow OA, but a discussion of surgical options for young dogs with elbow dysplasia is appropriate first.
Dogs typically present with lameness associated with elbow dysplasia between six and 18 months of age.
CT is the gold standard for identification of the different types of elbow dysplasia, while plain radiography remains a mainstay in the general practice environment. Once a diagnosis of one or more conditions is established, surgical treatment options may be considered.

Medial coronoid disease often involves fragmentation of the medial coronoid process tip. Surgical treatment typically involves fragment removal to improve comfort (the “stone in the shoe” analogy) and/or removal of some of the coronoid process deep to the fragment.
By taking more than just the fragment, surgeons aim to prevent future re-fragmentation, and reduce theorised impingement between the coronoid process and medial part of the humeral condyle (impingement is evidenced by abrasion of the articular cartilage in this region).
This is achieved through arthroscopy or arthrotomy.
OA progresses despite arthroscopic intervention and this may be the reason outcomes are inconsistent for arthroscopic treatment.
Medial coronoid disease exists as a spectrum of features. Some cases may be more likely to respond to certain treatments (for example, dogs with radioulnar incongruity or higher levels of cartilage wear may respond better to arthroscopic treatment; Barthélémy et al, 2014), but algorithms for selecting appropriate candidates are not in existence, as the evidence base for stratifying cases is not yet established.
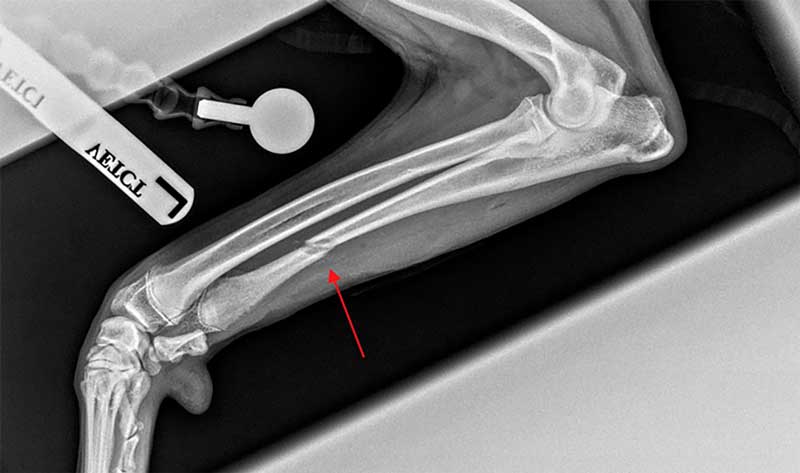
Radioulnar incongruity (Figure 1) is often addressed by osteotomy of the ulna.
Transection of the ulna allows realignment of the proximal ulnar segment and radius. The movement between radius and ulna is somewhat more complex than a simple proximal movement of the proximal ulnar segment (Böttcher et al, 2013). It is directed through:
Intuitively, this would suggest load sharing between the radial head and medial coronoid process would, to some extent, be restored. Ulnar osteotomies (Figure 2) are typically dynamic (that is, not plated), although plated ulnar osteotomy also exists (see the following passage in this article).
Improving load distribution in the joint should, theoretically, reduce the rate of OA progression, although, improved clinical function has only been demonstrated to date in a retrospective study using subjective outcome measures (Caron and Fitzpatrick, 2016).
Debridement is the treatment of choice for osteochondrosis, combined with various forms of disruption of the subchondral bone to encourage haemorrhage and infilling of the defect with fibrocartilage (which is considered superior to exposed subchondral bone). This is performed by arthrotomy or arthroscopy.

Osteochondral autografts acquired typically from the patient’s stifle and synthetic polyurethane plugs may also be used to fill sizeable osteochondrosis defects.
Treatment of ununited anconeal process (Figure 3) can involve fragment removal. However, the anconeal process is a primary stabiliser of the elbow joint during extension (that is, when the elbow is loaded).
As such, preservation of the anconeal process is preferred and can be achieved, in situations where its remodelling is not too severe, through lag screw fixation to the proximal ulnar metaphysis.
Combination of fixation of the fragment with dynamic ulnar osteotomy is recommended since part of the aetiology is thought to be radioulnar incongruity and resultant impingement between the humeral condyle and the anconeal process.
In the author’s approach to the young dog with elbow dysplasia, the recommendation to employ surgery is often based on the severity of the clinical signs, rather than the imaging findings.
The aims of surgical intervention should be:
An evidence base that any of the interventions consistently achieve these aims is currently lacking.

Part of the difficulty with generating evidence for surgery is the degree of variability within the diseases. Stratifying groups and generating meaningful data is complicated.
Furthermore, a high percentage of dogs undergoing, for example, arthroscopic coronoid surgery will show future lameness as a result of their OA. So, perhaps the data to prove the efficacy of surgical intervention is lacking because it is not efficacious.
Before totally discounting surgery for cases with elbow dysplasia, it is worth remembering that some dogs demonstrate a significant and sustained improvement in clinical function following arthroscopic subtotal coronoid ostectomy (and other procedures).
Identifying which dogs will benefit is difficult, though skeletally immature dogs are considered better candidates for joint interventions, perhaps because they have a greater capacity for remodelling of the articular contours and cartilage. Additionally, if little scope exists for improving the clinical picture because of mild signs, surgical intervention might not be in the dog’s best interests, while, with severe clinical signs, more potential exists to achieve improvement.
No matter what treatment is performed in the skeletally immature dog, elbow OA is inevitable.
Signs include lameness, elbow effusion/periarticular thickening, reduced elbow range of motion and resentment to flexion and/or extension. Imaging often reveals periarticular mineralisation (Figure 4), and the severity of this is correlated with the extent of articular cartilage loss when graded arthroscopically (Farrell et al, 2014).
Medial compartment disease is a stage of elbow OA in which the medial aspect of the elbow joint (medial coronoid process and medial part of the condyle) demonstrates articular cartilage loss, while the lateral aspect of the joint (radial head and lateral part of the condyle) demonstrates minimal cartilage loss (Figure 5).

The medial and lateral elbow compartments are, of course, continuous, and so OA in one side will always be shared by the other side. However, OA in the medial compartment advances more quickly than in the lateral compartment.
Lameness is often present following rest following exercise, but it is also reasonably frequent for animals to present with acute worsening of mild or non-existent lameness. Such episodes are termed “flare-ups”. A flare-up is not necessarily an indication for intervention. However, surgical options exist for elbow joints with advancing OA.
Two approaches for surgical management of medial compartment disease co-exist.
Dynamic ulnar osteotomies, plated ulnar osteotomies and a plated humeral osteotomy have been described to shift loading within the elbow joint.
The dynamic ulnar osteotomy does not shift load from the medial aspect to the lateral aspect; rather, it (theoretically) balances loading in the joint.
The proximal abducting ulnar osteotomy (PAUL) involves a transverse osteotomy of the ulna just distal to the elbow joint and application of a stepped plate to achieve abduction, caudal tipping and internal rotation of the proximal segment. However, in a mechanical testing study, pressure did not appear to be shifted from the medial to the lateral compartment, unless elbows were incongruent before surgery (McConkey et al, 2016).
The sliding humeral osteotomy involves a transverse osteotomy of the mid-shaft of the humerus and application of a stepped plate to induce medial translation of the distal segment. Initial literature demonstrated a high complication rate, although a later study showed a significant reduction in complications (Fitzpatrick et al, 2015). Although reasonable outcomes have been documented (Wendelburg and Beale, 2014), this procedure is not widely performed.
The major problems with uptake of these weight-shifting techniques are three-fold: candidate selection is complicated (the lateral compartment needs to be in reasonable health); complications may be severe (this is concerning – particularly since dogs are usually affected bilaterally by elbow OA); and outcomes compared with arthroscopy alone may be comparable.
The design of total elbow replacement systems is complicated (Panel 2). Replacing the medial compartment alone avoids the concerns of finding the balance between too much and too little linkage. Two main partial elbow replacement systems exist in the veterinary world.
The elbow joint is not a simple hinge. The humeroradial and humeroulnar joints have some varus/valgus laxity during normal elbow motion.
Also, rotational and proximodistal movements occur between the radial head and ulnar coronoid processes.
Linked prostheses, in which the humeral and radial/ulnar components act as a true hinge, result in significant stress at the prosthesis-bone interface, as all these other movements are resisted.
Unlinked prostheses reduce stress on the bone-implant interface, but rely on competence of the surrounding soft tissues (collateral ligaments, joint capsule and muscles) to maintain alignment. These soft tissues are often abnormal as a result of the degenerative joint disease and/or damaged during implantation, depending on the surgical approach.
“Semi-constrained” systems involve two linked components with a “sloppy hinge” connection and are intended to avoid the previously mentioned concerns. An alternative is to replace only part of the joint.
The canine unicompartmental elbow replacement (CUE) consists of a polyethylene bead placed into the centre of the medial coronoid process, just proud of the articular surface, which articulates with a metallic runner placed similarly proud of the articular surface of the medial part of the humeral condyle. The two components articulate through the majority of the joint motion.
Because this is a non-linked implant, bone-implant interface strain is minimised. Outcomes have been published in two studies. Cook et al (2015) documented catastrophic complications in 1%, major complications in 11% and outcomes including full function in 47.6%, acceptable function in 43.7% and unacceptable function in 8.7%.
Bayer et al (2019) documented major complications in 15% and outcomes including full function in 25%, acceptable function in 73% and unacceptable function in 1%.
The biomechanically anatomic nonconstrained and compartmental unicompartmental elbow replacement (BANC, Kyon Veterinary Products, Switzerland) is in development. The implant is intended to hinge in the sagittal plane, but also preserve pronation and supination.
Very few clinical cases exist and data regarding outcomes is limited.
Two surgical options exist for end-stage elbow OA.
Various systems have been devised for dogs; however, none has enjoyed wide uptake, as opposed, for example, to canine hip replacement. This speaks volumes about outcomes.
A 2016 retrospective study (De Sousa et al) of total arthroplasty of the elbow (TATE) revealed 24% full function, 52% acceptable and 24% unacceptable function on surgeon-assessed follow-up.
Owner (validated) questionnaires found consistent reductions in pain scores in comparison with the preoperative state, but no changes were recorded in mobility scores.
This involves removal of the articular surfaces of the elbow and application of implants to maintain a comfortable standing angle (approximately 135°) during fusion of the joint.
Clearly, salvage procedures for the elbow (arthroplasty and arthrodesis) carry reasonably high risks of major complications and, at best, adequate outcomes.

In addition, contralateral elbow disease is likely to be present in a high proportion of cases. Therefore, these procedures are only likely to be available to the most severely affected dogs.
The clinician should adopt a consistent approach to communication of non-surgical management of OA. The author describes a three-pronged approach: exercise modulation, bodyweight optimisation and medications/analgesia.
Advice regarding exercise should be to maximise the activity without unduly exacerbating the clinical signs of lameness. No evidence exists that exercise will increase the rate of progression of OA (this will continue at its own rate mediated at the cellular level). On the contrary, it is understood that:
Therefore, exercise is to be encouraged, affording dogs a superior quality of life in comparison with previous advice to avoid activity to minimise lameness. Mild lameness is to be expected, but does not indicate a welfare concern.
The influence of the adipose-derived inflammatory mediators on the clinical signs of OA is well documented, as are the benefits of body fat reduction on joint function in people with high body fat content.
Despite the protestations to the contrary from the pet-owning public, an appropriate diet is more important than the exercise regimen in maintaining a healthy body fat content. Appropriate advice and support should be given to clients, so that an optimal bodyweight may be achieved.
Analgesic medications include the NSAIDs grapiprant and bedinvetmab as first-line, regular treatments. The addition of tramadol, gabapentin and amitriptyline can be considered for short-term management of flare-ups of the clinical signs. The reader is encouraged to investigate the limited evidence-base supporting the various supplements for OA management in animals and humans.
A diet with a high ratio of omega-3 to omega-6 fatty acid content should be recommended (Roush et al, 2010). Other nutraceuticals may be of limited value.
Analgesia techniques can also involve physiotherapy (such as regular passive range of motion exercises, cool or heat compression application prior to and/or following exercise) and acupuncture. Limited evidence exists for intra-articular administration of autologous platelets, stem cells or hydrogels such as polyacrylamide; however, these may be of use in some cases and carry little risk of worsening the disease or clinical signs.
Elbow OA is a common disease and can have a detrimental effect on quality of life. While medial compartment disease gives us a window of opportunity for intervening conservatively and/or surgically, it should be considered only a stage in the progression to more severe OA.
Client education is instrumental in decision-making. Management options are increasing in number, but no single option can be expected to be appropriate for every case, as a result of a wide variation in the severity of disease.