3 Apr 2017
Sarah Caney discusses this common complaint in felines and suggests several possible treatments and management tools.
Sarah Caney
Job Title
Figure 1. Administration of SC fluids can be helpful in maintaining hydration in some cats with chronic kidney disease.
Chronic kidney disease (CKD) is one of the most common diagnoses made in clinical practice. A key to successful management is seeing your patients regularly and ensuring you allow sufficient time to perform a thorough evaluation.
Reinforcing key messages about treatments helps to support compliance to diet and medication. Attention to detail and good team work with the cat’s owner helps to achieve a good quality of life for years in many cases.
Treatment aims to help the patient compensate for its renal disease, allowing it to live for as long as possible with as good a quality of life. The most proven treatment is feeding a prescription renal diet, but many other supportive and symptomatic treatments could be helpful to individual patients.
Treatment should be focused on:
Treatment needs to be tailored to the individual according to its specific needs and those of its owner. Since CKD is a progressive condition, the needs of an individual patient are expected to change over time.
The most proven general treatment for CKD is feeding a specially designed renal diet. Studies have shown feeding one of these diets improves quality and length of life of affected cats. Renal diets are modified in a number of ways to support cats with CKD, with phosphate restriction considered the most important factor.
In normal cats, much of the excess phosphorus consumed in the diet is excreted by the kidneys and renal excretion of phosphate is dependent on glomerular filtration. Therefore, cats with CKD are vulnerable to phosphate retention and hyperphosphataemia.
Hyperphosphataemia and reduced renal production of calcitriol contribute to the development of renal secondary hyperparathyroidism. Unless treated, renal secondary hyperparathyroidism progressively worsens. High levels of parathyroid hormone (PTH) are thought to contribute to the uraemic state through acting as one of the uraemic toxins. High levels of PTH also contribute to ongoing renal damage through causing calcium influx into renal tubular cells and precipitation of calcium phosphate in the lumen of the tubules. Renal secondary hyperparathyroidism is seen in most – if not all – cats with CKD and may precede azotaemia.
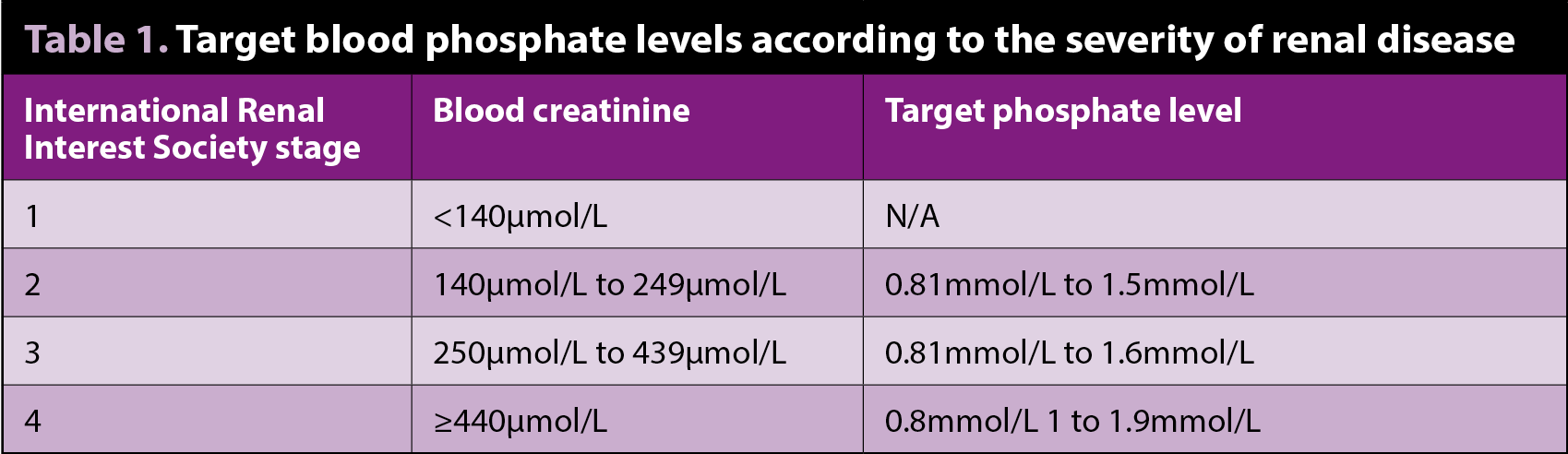
Phosphate restriction, through use of a renal diet and/or phosphate binder, is effective in preventing/reversing renal secondary hyperparathyroidism and hence slowing progression of CKD. The International Renal Interest Society (IRIS) recommends phosphate restriction for all cats in IRIS stage two, three and four CKD, irrespective of their blood phosphate levels. IRIS has also produced guidelines on target phosphate levels for cats with CKD (Table 1).
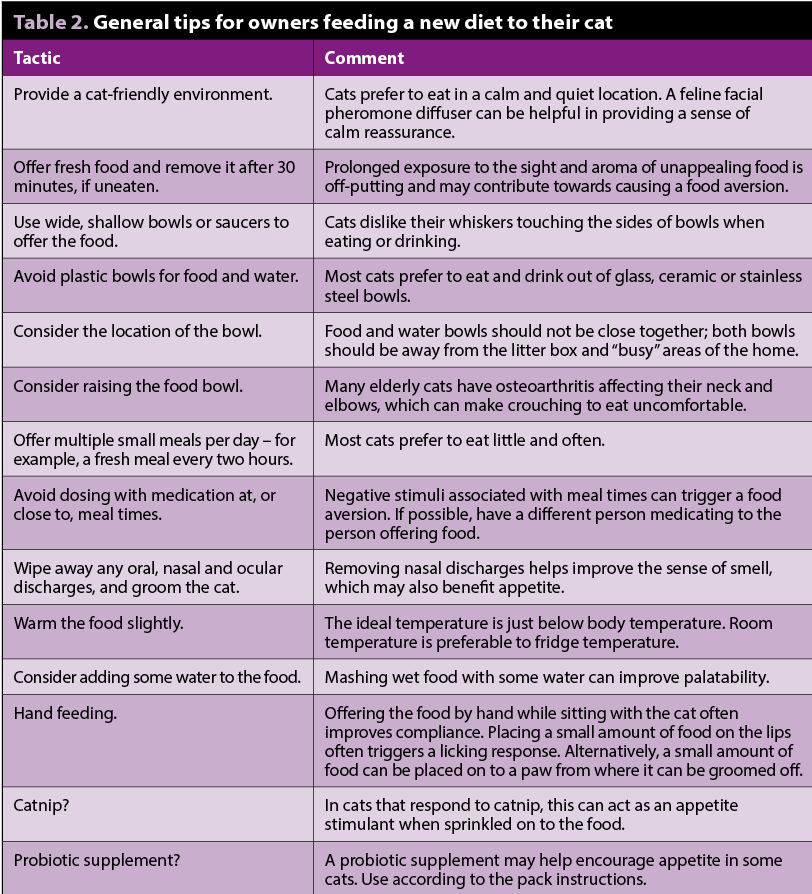
Renal diets should be introduced gradually – over weeks or months – to encourage long-term acceptance by the cat. General tips for encouraging a cat to eat a new diet are included in Table 2. It is always more important the cat eats, so if it is not interested in the prescription diet it should be offered food it will eat. Senior diets are preferable to routine cat food as these have lower levels of phosphate in them.
If feeding a renal diet is not possible, phosphate restriction can be achieved through the use of intestinal phosphate binders. Veterinary phosphate binders include calcium carbonate-containing products. Intestinal phosphate binders should be mixed with the food – they work by binding to phosphate present in the diet, retaining this in the bowel and limiting the amount of phosphate that can be absorbed by the body. In those patients with blood phosphate results higher than the IRIS targets, both a phosphate-restricted diet and intestinal phosphate binders may be required to attain adequate control, and it may take several months to achieve this.
Clients should be actively supported throughout the dietary transition period – follow-up telephone calls and consultations can help to troubleshoot reasons for poor compliance, provide support and educate the owner as to the dietary change that has been recommended. A published owner survey confirmed the importance of the veterinary recommendation for a change to a renal diet in cats with CKD. Of 859 owners of cats with CKD, those aware of a veterinary recommendation to feed a renal diet were 10 times more likely to be feeding any renal food compared to owners that had not received (or were not aware of) a veterinary recommendation to feed a renal food (Caney, 2016).
Common causes for poor dietary compliance include reduced appetite due to complications of CKD, such as dehydration, anaemia, electrolyte disturbances (such as hypokalaemia) and nausea. Symptomatic management of these complications should be considered in all CKD patients with a poor appetite. If all known complications of CKD have been addressed then an appetite stimulant treatment trial can be considered.
Loss of nephrons leads to activation of the renin angiotensin aldosterone system (RAAS), which results in hypertrophy of residual nephrons with reduced arteriolar resistance and increased glomerular blood flow.
As renal disease progresses, the afferent arteriolar tone decreases more than the efferent arteriole tone resulting in glomerular hypertension and hyperfiltration. Although this increase helps support glomerular filtration rate (GFR) and excretory function, ultimately RAAS activation has negative consequences, including proteinuria, renal damage, fibrosis, and further progression of renal disease. Angiotensin II is responsible for many of the damaging effects of RAAS activation.
Two veterinary licensed options exist for the suppression of the RAAS in cats with CKD:
IRIS recommends CKD patients are classed as proteinuric if their urine protein to creatinine ratio (UPC) is more than 0.4 and borderline proteinuric if their UPC is between 0.2 and 0.4. RAAS suppression using telmisartan or benazepril has been shown to be effective in reducing proteinuria, although a survival benefit has not been shown yet.
Some clinicians advocate treating borderline proteinuric cats (UPC 0.2 to 0.4) on the basis survival times in these cats are reduced compared to non-proteinuric CKD cats (UPC below 0.2) and this is considered logical by the panel responsible for the ISFM consensus guidelines on diagnosis and management of CKD (Sparkes et al, 2016).
ACEIs and ARBs should only be used in clinically stable, normally hydrated cats. There may be some benefits in treating non-proteinuric CKD patients with an ARB or ACEI since some studies have shown improved quality of life and a tendency for the renal disease to progress more slowly in these cats (King et al, 2006; Mizutani et al, 2006; Zimmering et al, 2014; Zimmering, 2015).
Telmisartan has a potential advantage over an ACEI by not being susceptible to “ACE escape” – the phenomenon whereby alternative pathways allow angiotensin II to continue to be produced in spite of administration of an ACEI. Telmisartan also offers a more targeted mode of action, sparing the AT-2 receptor, which may mediate some beneficial effects. A field study of cats with CKD showed telmisartan was effective in significantly reducing proteinuria at all assessment points in the 180-day study, whereas benazepril was not (Sent et al, 2015).
Dehydration is associated with reduced renal perfusion, which causes a worsening in renal function. Acutely decompensated cats require IV fluid therapy at a veterinary clinic, but maintaining adequate fluid intake at home is of prime importance. Cats with CKD should be encouraged to drink as much as possible, through tactics such as feeding moist, rather than dry, foods. Detailed advice on how to encourage voluntary fluid intake is available from www.vetprofessionals.com
In cats that fail to maintain adequate voluntary fluid intake, some owners may be willing to administer SC fluids at home (Figure 1). A typical regime involves giving 50ml to 100ml of Hartmann’s solution daily.
Many cats with CKD suffer from uraemic gastritis contributing significantly to their inappetence and weight loss. General nursing techniques, such as feeding warm food by hand and other tips presented in Table 2, may help.
In other cases, it is worth trying antacids (H2-antagonists such as famotidine 0.5mg/kg daily or on alternate days), antiemetics (such as maropitant 0.5mg/kg to 1mg/kg once daily) and/or appetite stimulants (such as mirtazapine 1mg/cat to 2mg/cat every other day or cyproheptadine 1mg/cat once or twice daily). In cats that are bright and relatively well, but where appetite remains poor, one long-term possibility includes placing a feeding tube, such as an oesophagostomy or gastrostomy tube.
Hypokalaemia (potassium below 4mmol/L), caused by inappropriate loss of potassium in the urine and inadequate intake due to inappetence, is present in around 25% of cats with CKD.
The cardinal sign of severe hypokalaemia is polymyopathy, with generalised muscle weakness and ventroflexion of the neck (Figure 2). However, more mildly affected cats will only suffer from non-specific signs, such as lethargy, weakness and loss of appetite. Hypokalaemia is not only a cause of clinical signs, but it also adversely affects renal function.

Potassium gluconate at a dose of 1mmol to 4mmol twice daily is the preferred oral supplement as it is the least gastric irritant. Renal diets – which are supplemented in potassium, but also are non-acidifying and low in protein – help to maintain normal serum potassium concentrations.
Systemic hypertension affects at least 20% of CKD patients. Hypertension can have serious consequences, including blindness, neurological signs, cardiac changes (most commonly a systolic heart murmur due to cardiac remodelling) and renal damage.
Blood pressure should be evaluated as a routine part of all check-ups of CKD cats and anti-hypertensive therapy prescribed to those where the mean systolic blood pressure readings, taken with the cat in a calm state, are persistently above 160mmHg, or where there is evidence of hypertensive retinopathy.
The most commonly used drug for treatment of feline hypertension is calcium channel blocker amlodipine besylate (0.625mg/cat to 1.25mg/cat once or twice daily). Angiotensin converting enzyme inhibitors, such as benazepril (0.5mg/kg once or twice daily), and ARB telmisartan may be effective for mild cases (systolic blood pressure 160mmHg to 180mmHg). In general, amlodipine is very effective as a sole treatment. In some cats, a combination of amlodipine with benazepril/telmisartan may be required to achieve adequate control.
Progressive anaemia is common in CKD and can contribute to lethargy, inappetence, weakness and weight loss. In some cats, iron deficiency can contribute to the anaemia both through inadequate dietary intake and gastrointestinal blood loss. Treatment options that may be considered include iron supplementation (50mg to 100mg ferrous sulphate daily), anabolic steroids and recombinant human erythropoietin (Chalhoub et al, 2011).
Other treatments not discussed may be needed in the individual patient according to its needs and are discussed elsewhere (Sparkes et al, 2016). Concurrent illness is common in many CKD patients, so consideration should be given to performing investigations and/or treatment trials to address these, as appropriate.
Monitoring visits are very important to ensure owners are supported and that clinical problems are identified and treated promptly. The required frequency of check-ups varies according to the patient’s needs, but should initially be at least once a month.
All check-ups should include weighing the patient and assessing for clinical problems (such as dehydration). Blood pressure and laboratory monitoring should be checked according to the patient’s needs and owner’s concerns – the author measures blood pressure every 3 to 6 months and reassess blood and urine tests every 6 to 12 months, depending on the individual patient’s needs.
Treatment interventions not only improve quality of life, but some examples, such as phosphate restriction, have the ability to increase lifespan. The long-term outlook for cats with CKD is very variable ranging from a few weeks post diagnosis to many years. For many cats, once stabilised, their care is not difficult, time-consuming or stressful, and it is possible to provide good quality of life for months or years.