6 Feb 2017
Sally Birch discusses the case of five-month-old male entire domestic shorthair cat called Simon.
Sally Birch
Job Title
Your first case of the morning is a five-month-old male entire domestic shorthair cat called Simon.
Simon has been presented to you for further investigation of poor growth, occasional vomiting and poor appetite.
On examination, Simon is very lively, weighs 1.1kg and has a body condition score of 2 out of 9. Cardiothoracic auscultation was unremarkable and Simon was normothermic. He appeared to resent abdominal palpation, which revealed prominent “lumpy” intestines.
Initial investigations included a complete blood cell count that revealed marked neutrophilia; 35.3 × 10^9/L, reference interval (RI) 2.5 to 12.5 × 10^9/L and borderline anaemia (packed cell volume 24.7%; RI 26%t to 47%). No leukocyte or erythrocyte abnormalities were present.
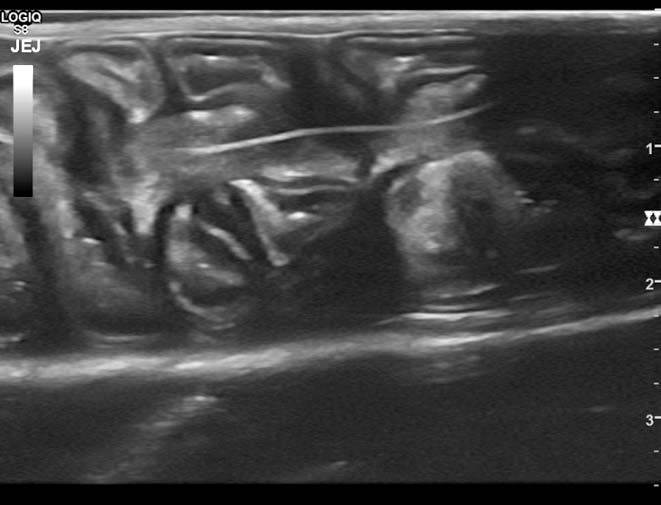
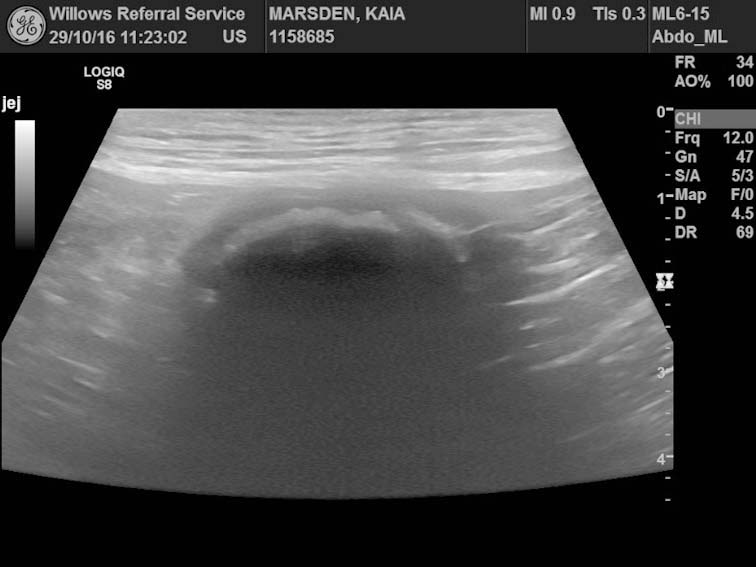
A serum biochemistry profile revealed mild hypoalbuminaemia (20g/L; RI 25g/L to 45g/L), but was otherwise unremarkable. A full abdominal ultrasound was also performed (Figure 1).
How would you interpret this ultrasound image?
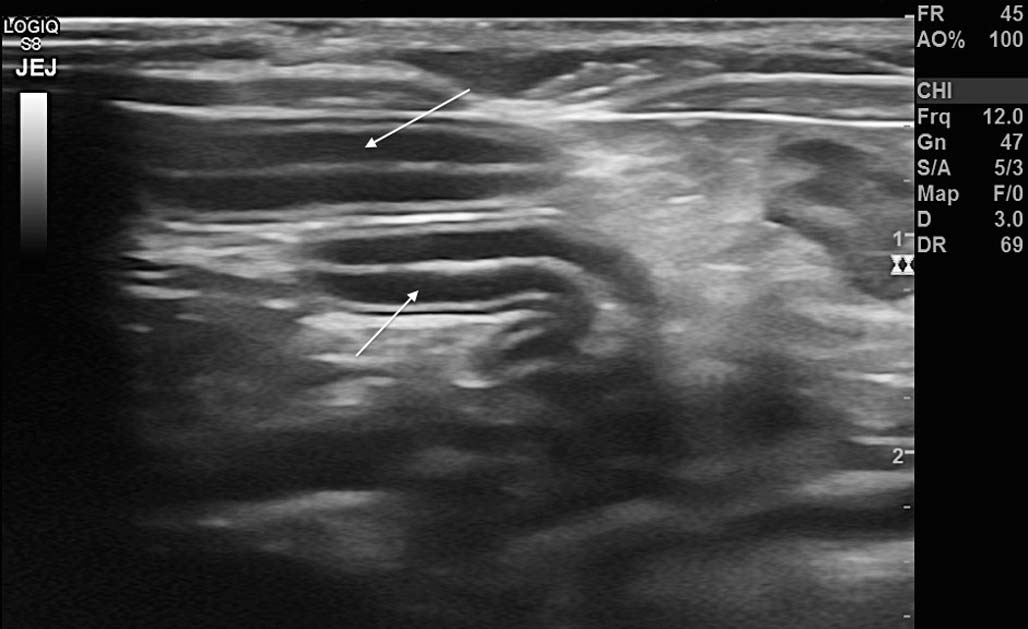
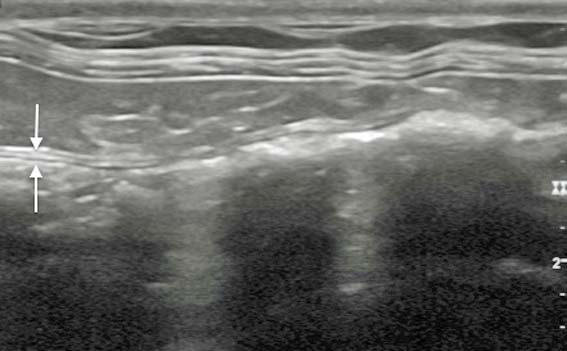
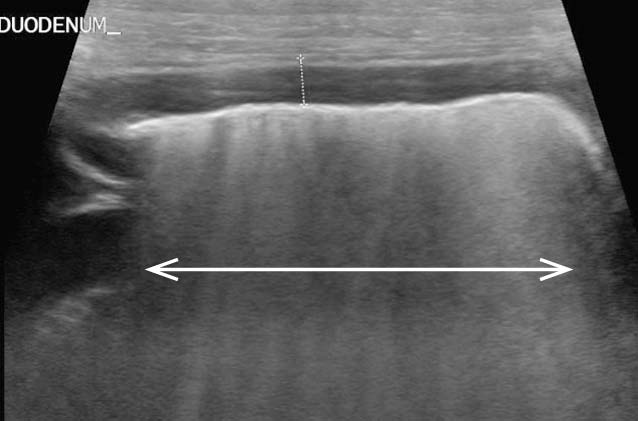
The ultrasound image shows a section of intestine. It is possible to determine this is small, not large, intestine from the appearance of the intestinal wall. The small intestine has a much thicker wall than the colon due, in part, to a much thicker mucosal layer (Figures 2a and 2b).
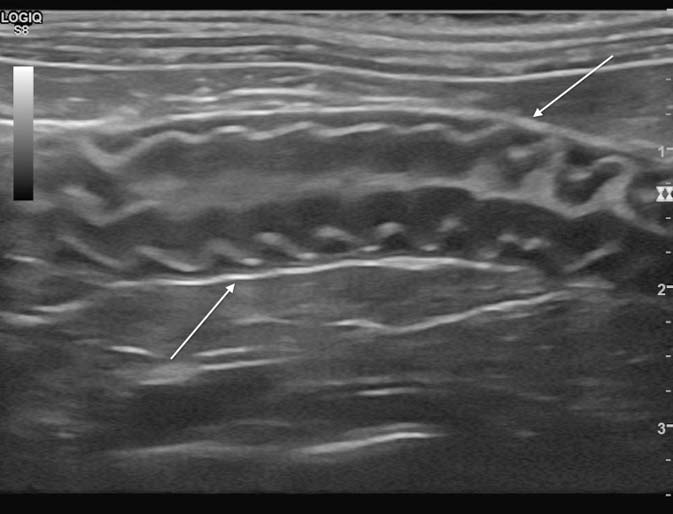
There is evidence of plication of the small intestine and a thin linear echogenic structure passing through the centre of the intestine (Figure 3). This structure could be traced proximally and could be seen entering the stomach and extending into the distal oesophagus (not shown). There is no evidence of small intestinal dilation.
The final diagnosis was a chronic small intestinal linear foreign body.
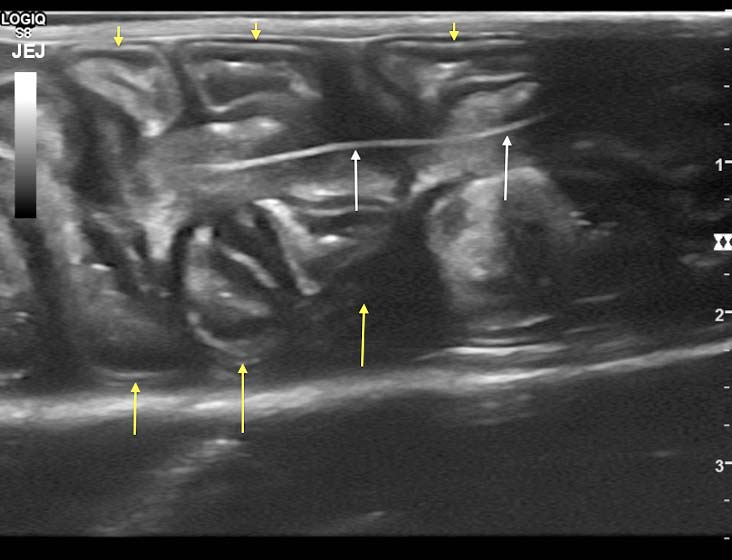
Intestinal plication should be differentiated from corrugation (Figures 5a and 5b). Plication occurs due to the presence of a linear foreign body and describes the appearance of an entire intestinal loop, including the serosa, forming hairpin bends while stacking adjacent to other loops. The term corrugation is used to describe intestine with a wavy mucosa and submucosa, but where the serosa remains straight. There are numerous differentials for this appearance, including peritonitis, pancreatitis, enteritis, intestinal infiltrative disease (neoplasia) and intestinal infarction.



When the presence of intestinal foreign material is suspected, a search for free gas and/or fluid should always be made to determine the likelihood of intestinal perforation.
A very small volume of anechoic peritoneal fluid was also present in Simon’s abdomen (not seen in image). This is not an uncommon finding in puppies and kittens, and is usually considered to be normal. If any doubt exists, or if the fluid is echogenic and sufficient volume is present, ultrasound-guided abdominocentesis can be performed to permit analysis of the fluid. The presence of increased echogenicity of fat within the abdomen, particularly surrounding the affected gut, should raise suspicion regarding the possibility of peritonitis.
Linear foreign bodies may also cause characteristic changes on radiographs. Typically, bunching of the intestines is seen and abnormally shaped gas lucencies may be present within the intestinal lumen (Figure 6). Care should be taken to distinguish this from the normal bunching of the intestines in the right side of the abdomen in cats with a large amount of intra-abdominal fat. A left-lateral view may reveal the presence of foreign material within the pylorus (more common in dogs).
Oral examination under sedation revealed the presence of a length of thread encircling the base of Simon’s tongue that extended distally into his oesophagus (Figure 7).
In cats, linear foreign bodies tend to anchor themselves around the base of the tongue, whereas, in dogs, foreign material is more commonly anchored in the pylorus, although overlap exists.
Exploratory coeliotomy was performed and revealed the linear foreign body had caused longitudinal sectioning of most of the small intestine from the duodenum to the caudal jejunum. An enterectomy was performed despite a guarded prognosis, Simon made a full and uneventful recovery and was discharged after several days following surgery.