29 Oct 2018
Katharine Nelson details the steps taken in the case of a domestic shorthair that presented with a superficial cat bite abscess and developed complications.
Katharine Nelson
Job Title
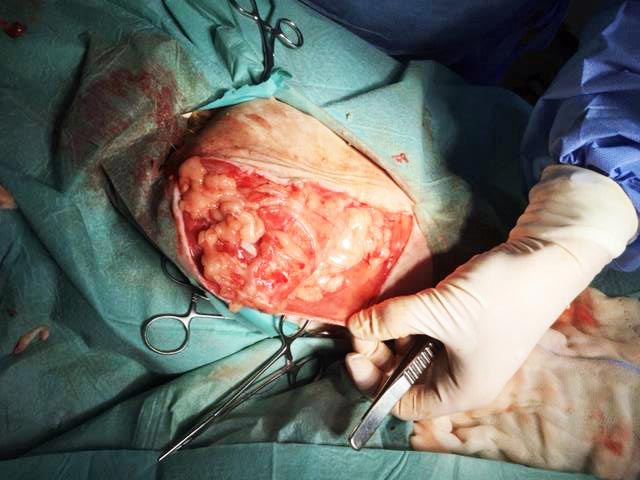
Figure 1. The large dead space left between the hindlimb musculature and the overlying skin.
A one-year-old male, neutered, domestic shorthair presented for evaluation of a superficial cat bite abscess affecting the lateral hindlimb, just proximal to the stifle.
The cat was discharged uneventfully following standard treatment (debridement and flushing under anaesthesia, followed by systemic broad-spectrum antibiotics), but deteriorated within a few days.
The cat represented 72 hours after the initial procedure with pyrexia (40.4°C); lethargy; anorexia; and a diffuse, painful swelling of the lateral and medial stifle, extending proximally towards the hip. The cat was hypotensive (90mmHg to 100mmHg). The respiratory rate was recorded as 28 breaths per minute, heart rate at 168 beats per minute and the mucus membranes were subjectively pale.
Haematological parameters were within normal limits, other than a mild neutrophilia (11.2 × 109/L, ref 1.48 × 109/L to 10.29 × 109/L). A fine needle aspirate was taken from the diffuse swelling and was found to contain many neutrophils. A diagnosis of extensive SC and IM abscessation with potential septic changes was assumed.
The cat was treated with IV fluids and IV antibiotics (co-amoxiclav and metronidazole), and a second anaesthetic was performed to explore the hindlimb swelling via a large lateral skin incision cranial to, and parallel with, the femur.
Approximately 40ml of purulent fluid was drained from beneath the skin, and between, and muscle bellies. This left a large dead space between the hindlimb musculature and the overlying skin, both medially and laterally around the upper hindlimb (Figure 1).
The tissues were flushed copiously with warmed saline and any necrotic areas of fat or fascia were debrided. The dead space was closed with tacking sutures (2M poliglecaprone 25), and Penrose drains were placed medially and laterally to allow ongoing drainage before the skin wound was closed routinely.
An oesophagostomy tube was placed to allow assisted feeding. Ongoing analgesia (meloxicam and methadone) and IV antibiosis were continued in the postoperative period.

The cat remained pyrexic and lethargic for a further 72 hours, with continued purulent discharge from the Penrose drains. Culture and sensitivity indicated the selected antibiotic regime was appropriate.
After 72 hours, the volume of discharge from the drains had reduced dramatically and the pyrexia was noted to have resolved (temperature 37.4°C).
The cat’s demeanour became noticeably brighter and it began to eat voluntarily. The oesophagostomy tube and Penrose drains were removed, and the cat was discharged to continue oral antibiosis and analgesia.
The cat was re-evaluated 14 days after the second surgery. The exploratory skin wound on the lateral thigh appeared to have healed routinely, with the exception of a 2cm ventral section through which a low volume of non-purulent, clear fluid was discharging (Figure 2).
The cat remained bright and the pyrexia had not returned. The leg was comfortable and no lameness was observed.
The infection had clearly resolved, but the wound was not healing.

Exploration revealed, although the majority of the skin wound had healed, no connection existed between the skin and underlying muscle of the entire proximal hindleg.
This type of wound is known as a pocket wound and occurs when the subcutis fails to cross-link with the underlying granulation bed.
In this case, the extensive destruction and debridement of SC tissue caused by abscessation and its management is likely to have been the major predisposing factor.
Bite wounds, wounds following major tumour resection, and wounds in inguinal, axillary and flank areas appear to be especially prone to pocket wound formation (Demetriou and Stein, 2011).
As the previous attempt to anchor the skin margins to the granulation bed and manage dead space with tacking sutures and drains had failed, an alternative solution was sought.
Omentalisation of non-healing wounds has been described in cats (Lascelles et al, 1998, 2001; Brockman et al, 1996) – primarily in axillary wounds, but also in the inguinal region.
The omentum is able to enhance circulation, drainage and healing, combat infection and encourage adhesion of the overlying skin to the granulation bed in these cases.
The cat underwent a third anaesthetic and the hindleg wound was again opened, debrided and flushed.
An omental flap was created at laparotomy by dividing the dorsal leaf of the omentum at its pancreatic attachments, then further lengthened by partially dividing the flap to create an “L” shape (Figure 3).
The omental pedicle was carefully tunnelled through the lateral body wall and beneath the skin to the wound.
The omentum was then wrapped around the muscle of the hindlimb, occupying the entire dead space between the hindlimb muscle and the overlying skin (Figure 4). Simple interrupted sutures of 2M poliglecaprone 25 were used to tack the tissues in position. The skin wound was closed routinely over the top.
The cat made an excellent recovery from surgery. The skin wound healed uneventfully and sutures were removed 14 days later.
No further wound breakdown or discharge occurred. A slight thickening remains palpable medially beneath the skin – ultrasonography revealed this is where several layers of the omental pedicle have adhered together, but the cat is asymptomatic and no further treatment is required.