5 Dec 2022
Harriet Hall, BVMedSci, BVM BVS, PGCert, MRCVS, discusses what such vaccines are for, schedules, as well as the importance of encouraging owners to vaccinate pets.
Harriet Hall
Job Title
Image: © Happy monkey / Adobe Stock
The way we recommend vaccinating our pets has continued to change over the past few decades.
It is estimated that only 30% to 50% of the pet population is vaccinated in developed countries, geographical pockets of infection remain and sporadic outbreaks of disease may occur1.

Though most people routinely vaccinating their pets still make an annual visit to their vet for a booster vaccination in the UK, tailoring the need for vaccination to the individual pet should be a consideration for practitioners – particularly when considering recent pressures on the profession, including the increasing UK pet population following the COVID pandemic, and the increased demand for vets/staff shortages following Brexit and the retention crisis.
How we vaccinate in small animal medicine is driven by three main factors:
Establishment of expert panels such as the WSAVA Vaccination Guidelines Group (VGG), which provides advice to the profession, were developed as a result of these factors. These guidelines provide a good scientific evidence base, but are intended to be adapted by practitioners.
Core vaccinations are defined as those that protect animals from severe, life-threatening diseases that have global distribution, and that all dogs and cats – regardless of the circumstances or geographical location – should receive (Panels 1 and 2)4.
Non-core vaccines are those that are required only by those animals whose geographical location, local environment or lifestyle places them at risk of contracting specific infections, and those vaccines that are not recommended are those where insufficient scientific evidence exists to justify their use or have restricted geographical availability or application (Panels 1 and 2)4.
Considering this, key questions for practitioners regarding vaccination in dogs and cats in the UK remain:
A good understanding of current epidemiology and specific diseases is necessary to answer these questions, and allow us to discuss and adapt the guidelines appropriately to individual animals.
Core
Non-core
Not recommended
Canine enteric coronavirus.
Determining what we should vaccinate against will also depend on individual circumstances, including whether the patient is a household pet, has access to the outdoors, is in a multi-pet family or in a shelter (kennels/cattery/breeding), has a necessity to travel and so on.
Assessing and, ideally, vaccinating the entire population of dogs and cats in the UK is challenging, but is still an important goal as vaccination is not just about protection for the individual, but protection of the population through establishing adequate herd immunity1.
Vaccination principles remain important – in particular primary courses given in advance of potential exposures and, wherever possible, booster vaccinations timed appropriately to optimise protection. Realistic expectations with regards to small animal vaccinations should be maintained and discussed with owners:
Infectious diseases with an available vaccine in the UK for dogs (core and non-core) include the following.
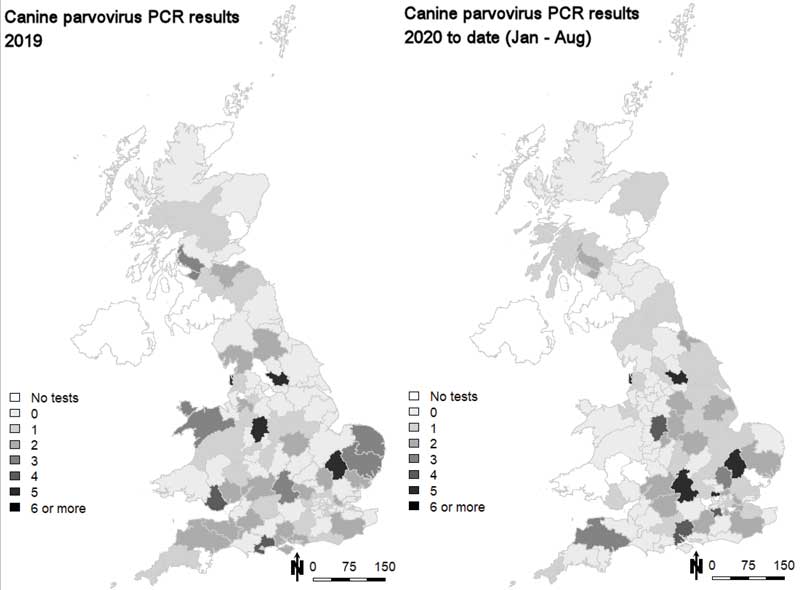
Parvovirus enteritis caused by canine parvovirus type-two is well established worldwide, and probably the most common infectious disease of dogs with high morbidity and mortality5.
Core
Non-core
Not recommended
* Not available in the UK
With classical clinical signs, the virus is able to induce mitosis in the cells it infects and, therefore, relies on the rapidly multiplying cells of the body – namely the thymus, bone marrow, spleen and crypt cells of the gut epithelium5.
Stress factors such as weaning and parasitic infections can predispose dogs to infection. Animal shelters are also considered to be at higher risk of infection. This is generally as these populations of animals are at a higher density, with high population turnover and a potentially unknown vaccination history4.
The importance of core vaccination and actively discussing this with owners – particularly following the COVID-19 pandemic – should be considered by practitioners when taking into account the rise in cases of parvovirus seen during this time.
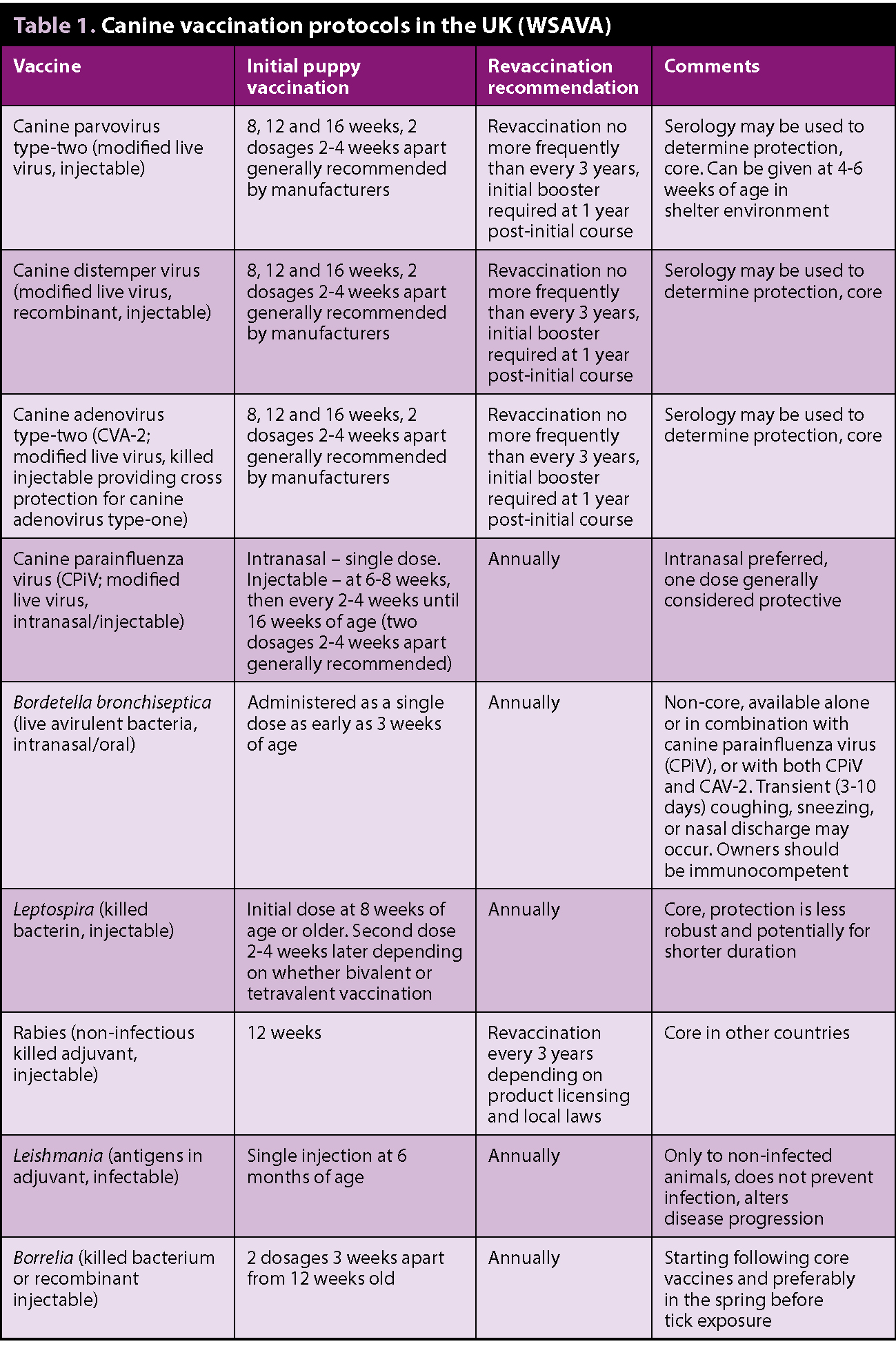
The most common cause of vaccine failure is interference from maternally derived antibodies – this underlies the current recommendations for vaccination every two to four weeks until 16 weeks of age by the WSAVA VGG (Table 1)4.
Canine distemper is an acute to subacute systemic contagious disease, with the causative agent being canine distemper virus (CDV)5. Capable of infecting a variety of species, CDV is seen rarely in UK veterinary practices today – largely considered to be due to vaccine protocols6.
Sporadic cases, however, are still reported, and concerns have been expressed regarding introducing the infection through pet immigration6. The more recent reported examples include two cases in puppies after rehoming in the south-west of the UK (the origin of infection was not determined7) and in a litter of puppies from a bitch imported from Bulgaria6 – highlighting the need to consider canine distemper as a differential diagnosis in cases with a travel history and suggestive clinical signs.
Outbreaks are also still considered possible in shelter facilities, with regional epidemics being reported in the past – some characterised with rapid spread, high morbidity and mortality5. Cases in wildlife (ferrets or foxes) have also been reported in the UK in the north-east in 2020 and a total of 67 positive PCR tests across various regions of the UK were also reported in dogs between January 2019 and August 20208.
Collectively, this indicates a need to continue vaccination as suggested by advisory groups (Table 1)4.
Serology can be used following vaccination for measuring CDV antibodies to assess level of protection and need for revaccination1,5. In kennels of a hospital environment, routine disinfection procedures are usually adequate in destroying CDV as it survives only short periods in the environment; is susceptible to inactivation with a number of disinfectants; and is susceptible to heat, UV light and drying5 (Panel 3).
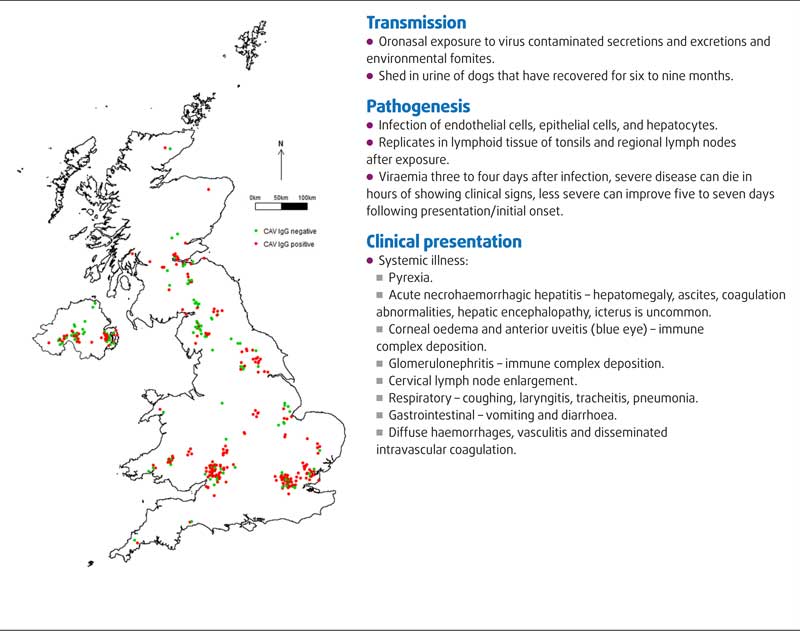
Infectious canine hepatitis is caused by canine adenovirus type-one (CAV-1), which has a close genetic and antigenic relationship with canine adenovirus type-two (CAV-2)5.
Transmission
Pathogenesis
Clinical presentation
Mammals that are most likely to contract and spread infection are foxes, wolves, coyotes and the domestic dog. It has a worldwide distribution.
The incidence of infectious canine hepatitis is low in developed countries due to core vaccination, though cases are still identified in unvaccinated puppies, wildlife centres and from imported cases9,10. It has also been reported that CAV-1 is endemic in red foxes in the UK in 2016 and shed in urine11, confirming their importance as a wildlife reservoir host and indicating that vaccination against this disease still has a place in the UK.
Practitioners should be aware that a risk of infectious canine hepatitis exists in unvaccinated individuals. Vaccines for CAV-2 are used to produce cross-reactive antibodies that elicit protection without the complications seen with the CAV-1 vaccines (corneal oedema5,10). Current recommendations for vaccination schedules are reported in Table 1.
Leptospirosis is a zoonotic bacterial disease caused by pathogenic species of the spirochete bacteria Leptospira, of importance worldwide in people and animals12,13. It is endemic in the UK14. Effective protection has not been shown to persist beyond 12 months as yet for any of the available vaccines in the UK12-15, and it is, therefore, appropriate to recommend vaccination annually in all dogs.
One report exists, however, using a tetravalent vaccine in the US that suggests immunity against the serovar grippotyphosa for at least 15 months16, so further research into duration of immunity is still required for all serovars to determine appropriate times between vaccinations.
Tetravalent vaccines have been available in the UK since 2013, providing immunity to serovars in four major serogroups (icterohaemorrhagiae, canicola, australis, grippotyphosa), which have been implicated in cases of canine leptospirosis in Europe.
Reports exist of cases of leptospirosis due to the australis serogroup isolated from dogs with nephritis in the UK14 and in dogs vaccinated with only bivalent vaccines in Europe; therefore, the use of tetravalent leptospirosis vaccines are recommended as per the European Consensus statement13.
Despite concerns that leptospirosis vaccines (particularly tetravalent) could be linked to development of anaphylactoid reactions in dogs after vaccination/higher risk of adverse events – particularly in small breed dogs1,12,13,17 – adverse effects for the use of both bivalent and tetravalent vaccines are deemed low and to be no more than other canine vaccinations4,12,17.
Dogs that are vaccinated for leptospirosis have variable MAT titres over time and antibodies should not be used to accurately predict resistance to Leptospira infection4,18.
Canine parainfluenza virus and Bordetella bronchiseptica are both part of the Canine Infection Respiratory Disease Complex (CIRDC), also referred to as kennel cough or tracheobronchitis5. CIRDC is characterised by acute onset of coughing with or without sneezing, nasal and ocular discharges can also occur depending on the infectious agent involved.
Outbreaks of respiratory disease occurs in dogs despite routine vaccination, and it should be remembered that co-infection with multiple pathogens is common19 and these pathogens are only part of a multifactorial process that also includes factors such as stress, immune status, previous exposure, ventilation and overcrowding5.
Vaccination does not prevent colonisation and shedding of the organisms and clinical signs can develop in vaccinated dogs, due to environmental pressures and given that all pathogens in the CIRDC are not represented in current vaccines5,19. Morbidity is generally reduced in those that have received a vaccine when exposed5,19. The intranasal preparations are generally preferred.
Lyme disease is caused by bacteria from the Borrelia burgdorferi (Bb) group and transmitted by Ixodes species ticks in the UK5.
Lyme disease is the most common vector-borne disease in Europe with a gradual increase in the number of reported human cases in the UK until 2018, at which point this approximately plateaued20.
Some pets are considered at a higher risk of leptospirosis and this consideration should be taken into account when discussing the need for vaccination in a particular dog with the following questions posed to owners:
Q. Has there been a period of high rainfall or flooding in a warm climate? Or has the pet been near stagnant waterways, rivers or lakes?
Q. Could the dog have encountered an area inhabited by rodents, foxes, hedgehogs, livestock (pigs, cattle, horses, sheep), or other unvaccinated dogs? (This may be more likely in a rural setting or if the dog is a working dog).
Q. Is the dog in kennels/in a shelter or kept with a large group of dogs?
Q. Is the dog a working dog or living in a rural area?
They have been reported to be at increased risk.
Although the incidence of clinical cases of Lyme disease in dogs has not been reported to increase, the prevalence of ticks infected with Borrelia in the UK has been suggested to be considerably higher than previous estimates have indicated21.
In Europe, Bernese mountain dogs have been reported to be more commonly seropositive for Bb in comparison to other breeds22. In people exposed to Bb presenting with clinical signs, only 10% are asymptomatic; in dogs, however, 95% are asymptomatic23. Clinical signs when present in dogs are characterised by lyme arthropathy and lyme nephropathy; neuroborreliosis is poorly characterised in dogs5,22,23.
Various controversy exists with differing opinions regarding vaccination against Bb. The only consensus reached is that no vaccine is required for those in non-endemic areas such as the UK23. This is primarily because Bb infections are commonly subclinical or respond rapidly to medical treatment. Those cases that develop severe clinical signs may have a genetic predisposition to immune mediated disease and vaccination with lyme antigen may not be the best for these dogs (post-vaccinational lyme nephropathy), and good tick control is required regardless in lyme-endemic areas due to other tick-borne diseases23.
Those who do recommend vaccination report high efficacy, safety and good duration of immunity, and the evidence for a negative impact of vaccination remains anecdotal at best22. Consensus for vaccination in endemic areas has not been reached. It is not recommended to vaccinate sick or proteinuric dogs.
Some veterinarians recommend vaccination in seronegative, healthy dogs in endemic areas and those that are healthy, but seropositive in high-risk areas that are non-clinical and non-proteinuric. All dogs in Bb-endemic areas should receive adequate tick control22.
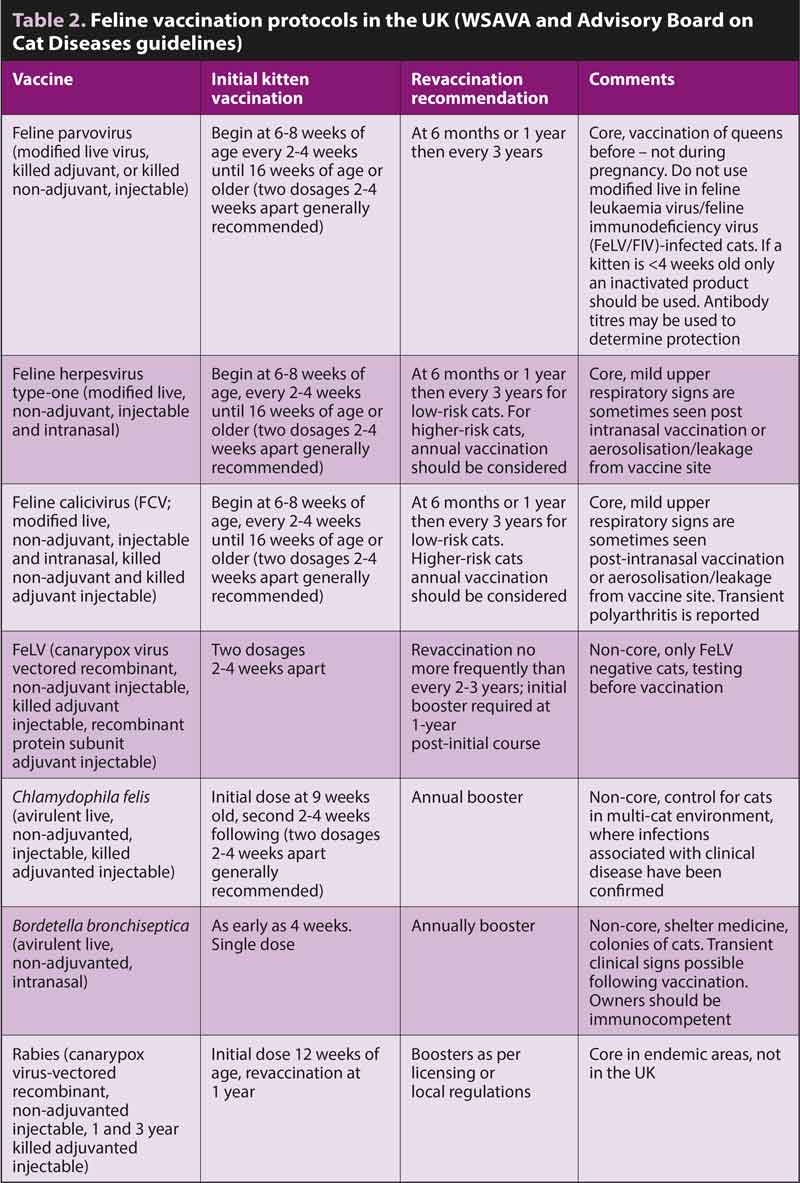
Feline herpesvirus (FHV) causes feline viral rhinotracheitis and has a worldwide distribution; it is often associated with FCV – both of which are the main primary pathogens in upper respiratory tract diseases in cats24, 25.
Latent chronic infection (lifelong carriers with the trigeminal ganglia being the site of FHV type-one; FHV-1 latent infection25) typically follows acute FHV infection, and intermittent reactivation (due to stressful events) allows viral shedding in oronasal and conjunctival secretions26.
Vaccination protects against disease and can reduce viral shedding following infection, but does not necessarily protect against infection. Despite vaccination, infections with both FHV-1 and FCV are particularly common when cats are kept in groups (such as shelters or multi-cat households); negative FHV-1 cats that have had suspicious clinical signs should be retested periodically due to lack of shedding in latent periods25.
Vaccination is advised on a risk-benefit basis, annually in cats at high risk and at three-yearly intervals in low-risk individuals – for example, in indoor single household cats24. Core vaccination in cats is recommended as per the European Advisory Board on Cat Diseases (ABCD) and the WSAVA VGG recommendations (Table 2).
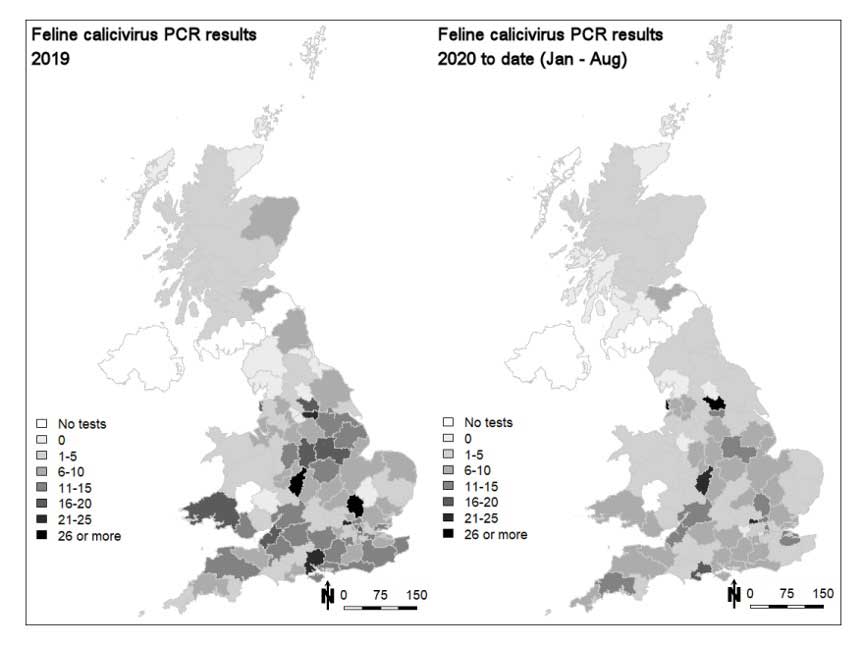
Feline calicivirus (FCV) continues to be prevalent in UK cat populations and is considered a primary pathogen in upper respiratory tract disease in cats, although more severe systemic forms of FCV infection have been observed27. Transmission between cats occurs via respiratory secretions, urine, faeces, fleas and aerosols.
FCV carrier state is defined as a cat shedding the virus for more than 30 days following infection. In a minority of cats, carrier state appears lifelong for FCV; however, most cats eliminate the virus at some point, but remain susceptible to reinfection5.
The virus persists in the tonsils and other oropharyngeal tissues, and shedding can be continuous in the carrier state though cycles of shedding appear more common, with this being approximately 10% of cats in the general population and up to 100% of cats in high-density populations5.
The main clinical signs of FCV include oral ulceration, upper respiratory tract signs, fever and chronic stomatitis/gingivitis. Cats with virulent strains of FCV present with pyrexia, cutaneous oedema, ulcerative lesions on the head and limbs, and jaundice27.
The prevalence of FCV is generally higher than FHV-1 in cases of upper respiratory disease in cats and FCV seems to play a more significant role25. FCV can rapidly mutate, evade the immune system and multiple strains of FCV can develop. Consequently, FCV strains found in vaccinations may not prevent field isolates found in the UK and older vaccine strains are potentially less effective28.
Core vaccination in cats is recommended as per the ABCD and WSAVA VGG recommendations (Table 2).
Feline panleukopenia virus (FPV) and canine parvovirus (CPV) are a single taxonomic entity, but FPV refers to parvovirus in cats29. Limited data exists that is available regarding the prevalence of FPV, although rescue shelters and breeding catteries are deemed to be at a higher risk30.
Classic acute disease
Atypical acute disease
Chronic disease
Other FHV-related disease
FPV causes 95% of cases; 5% are caused by CPV in cats31. The virus replicates in the tissues in the oropharynx and is distributed via viraemia initially to regional lymph nodes5. Common clinical manifestations include diarrhoea, lymphopenia, neutropenia, cerebellar ataxia and fetal death/loss of pregnancy29.
In most cats, maternal-derived antibodies remain protective until six to eight weeks of age. These often wane by 8 to 12 weeks; however, some kittens with poor maternally derived antibodies will be vulnerable earlier and some will fail to mount an immune response due to being still protected by maternally derived antibodies at 12 weeks29,32. Hence, later vaccinations have been described to have advantages as described in the ABCD and WSAVA VGG recommendations (Table 2).
Due to particular importance and re-emergence in shelter medicine, kittens should receive vaccinations against FPV earlier in these situations (four to six weeks). Antibody titres – using point of care test kits (ELISA or immune-migration-based) – can be used to assess protection in adult vaccinated cats and can, therefore, inform regarding re-vaccination and can be used in shelter medicine to support FPV outbreaks by identifying unprotected cats32.
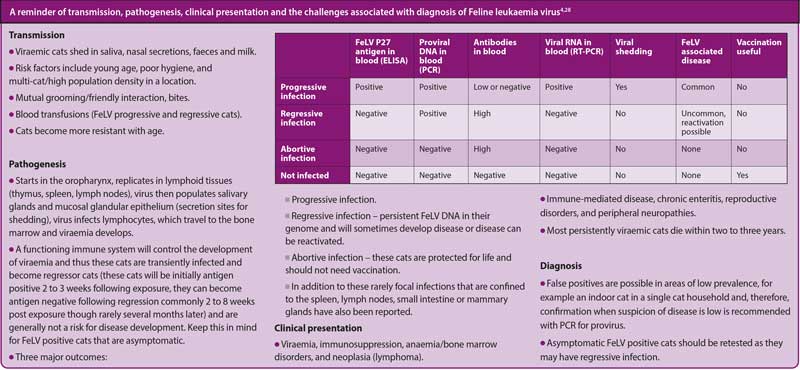
Infections occur worldwide, dependent on cat population density, geographical and local variation. In European countries, the prevalence in individually kept cats is commonly less than 1%. In multi-cat households with no specific preventive measures in place, the prevalence of feline leukaemia virus (FeLV) may exceed 20%33. All cats with an uncertain FeLV status should be tested prior to vaccination. Vaccination is recommended in all at-risk cats according to current ABCD and WSAVA VGG recommendations (Table 2).
B bronchiseptica is a Gram-negative bacterium that colonises the respiratory tract and is a primary pathogen of domestic cats. Particular attention should be given to situations of high population density (shelters or multi-cat households). Dogs with B bronchiseptica infections pose a risk for cats; clinical signs include fever, coughing, sneezing, ocular discharge, lymphadenopathy and pneumonia.
Identification using B bronchiseptica PCR in bronchoalveolar lavage samples of cats is diagnostic. Non-core vaccination with an intranasal product for cats is available, but should be limited to cats at high-risk or living in high-density populations34.
Chlamydophila felis is a primary conjunctival pathogen and concurrent upper respiratory tract signs are infrequent in cats35. Young animals are particularly susceptible to infection. Classical clinical signs can be unilateral or bilateral, and include serous ocular discharge, blepharospasm with a hyperaemic and chemotic conjunctiva35.
Though C felis is a non-core vaccination, antigens are always incorporated into combination vaccines in the UK, but would only be recommended in cats in high-density populations (shelters, breeding catteries or stray cats) with the primary goal being to lessen the potential for clinical disease in cats that are exposed.
Limited information is available regarding immunity following vaccination, but a reduction in clinical signs after challenge has been demonstrated at one year36. Limited evidence exists that the organism may be transmitted between cats and people (particularly those that are immunocompromised)37,38, which has also been used as a justification for vaccination.