21 Nov 2016
Ariane Neuber considers the causes of skin allergy in dogs, including ectoparasites, bacteria, environmental factors and stress, and measuring the patient’s pruritus threshold.
Ariane Neuber
Job Title
Figure 7. Microscopic view of a parasite from a dog.
Allergic skin diseases are commonly diagnosed in companion dogs and one of its main presenting signs, pruritus, is one of the main reasons for visits to first opinion veterinary practices (Figure 1).

Canine atopic dermatitis (CAD) and flea allergic dermatitis (FAD; Figure 2), as well as food-triggered allergies, are very common.
Many articles have been written about the diagnosis and treatment of canine cutaneous hypersensitivity. The pathogenesis is very complex and involves barrier function defects, aberrant immune responses, and environmental factors, to name a few.
The diagnostic process needs to focus on ruling out any differentials and, subsequently, identifying the allergens involved in the disease process. Treatment is aimed at allergen avoidance where possible, changing the misdirected immune response with the use of allergen-specific immunotherapy (if owners are willing to subscribe to the process), anti-inflammatory/antipruritic medication (if indicated), restoration of the skin barrier function as much as possible, and last, but not least, managing flare factors that need to be identified and addressed appropriately.

This article aims to shed more light on a very important, and sometimes overlooked and neglected, aspect of this group of diseases – flare factors.
In the author’s clinical experience, many a mildly affected patient improves dramatically when flare factors are handled well. Often antipruritic medication can be reduced significantly, may not be needed at all, or not at all times in cases with adequately controlled flare factors. Flare factors are mainly secondary infections, ectoparasites and dry skin.
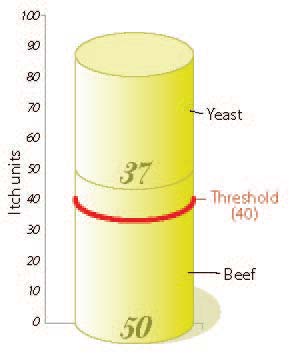
In the context of flare factors, it is very important to understand the concept of the pruritus threshold. This concept tries to illustrate the reasons why each patient with an allergic skin condition has waxing and waning levels of pruritus. Several factors contribute to the level of itch at any given time. If pruritus was measurable and itch units could be assigned, each patient would have a personal threshold above which clinical signs of itching, such as scratching, licking, over-grooming and rubbing, can be seen. Different variables can contribute to the summated itch units and bring the patient over its threshold.

For argument’s sake, the two-year-old male neutered Labrador retriever (patient A; Figure 3) you have diagnosed with CAD today, may have presented to you because it has a mild allergy to house dust mites, which may give it a score of 20, as the levels of house dust mites are low in the house and, in addition, it has got a flea infestation – giving it a score of 35. The family has recently moved house with the stress leading to an additional 10 itch units. Its personal pruritus threshold is 50, meaning it is showing clinical signs and needs treatment at this stage.
This equation may look very different for patient B (Figure 4) – a five-year-old female neutered West Highland white terrier, which has beef-induced CAD, and recently managed to steal a steak off the barbecue (resulting in 50 itch units) – leading to a secondary yeast infection (add 37 itch units). Patient B is not on flea control, and picking up some parasites in addition to the already high itch unit score – well above the personal threshold of 40 – would lead to serious quality of life issues.
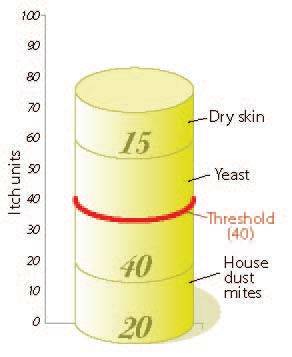
Patient C (Figure 5) is a two-year-old, female neutered Labrador retriever with very dry skin (15 itch units), Malassezia overgrowth (40 itch units) and is allergic to house dust mites (20 itch units). Once the yeast overgrowth is under control, this patient should be well-controlled and comfortably below its threshold of 40.
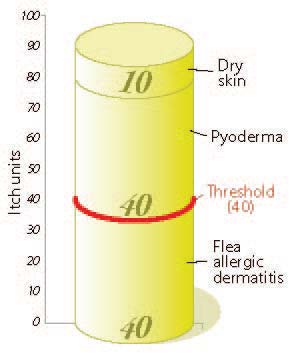
Patient D (Figure 6), a six-year-old male entire German shepherd dog, has got FAD in the face off a very low flea infestation (40 itch units), as well as dry skin (10 itch units) and a secondary bacterial pyoderma (40 itch units). In total, this score is well above its threshold of 40 and urgently needs treatment of all the factors involved.
These calculations illustrate the importance of dealing with, and ideally preventing, flare factors to give patients with CAD a good quality of life.

Unfortunately, allergic patients are not immune to parasites (Figure 7). Some dogs are allergic to fleas and their flea control needs to be above board anyway. In addition, many allergic patients suffer from multiple allergies – for example, they are allergic to house dust mites as well as fleas, to weed pollens as well as ingested beef and dairy product – or any other combination of possible allergens.
Cross reactivity exists in serological tests to house dust mites and Sarcoptes IgG. It is, therefore, conceivable such a cross reactivity also exists in vivo. Although the old paradigm one bite can set off flea-allergic patients is not necessarily true, flea-allergic individuals and, probably, allergic individuals in general, cannot cope as happily with flea bites, as dogs with no degree of hypersensitivity reaction; therefore, and for a number of other reasons, these patients require a different strategy when it comes to flea control.
If no evidence of fleas can be seen on the patient, it does not rule out their presence in the animal’s environment. Studies with flea-allergic cats have shown increased grooming behaviour leading to loss of evidence of the fleas’ presence; however, the allergic insult occurs, despite the lack of signs that the “culprits” are present.
It is, therefore, very important to explain the basics of flea biology to dog owners affected by CAD to motivate them in to keeping up good flea control at all times. Fleas are survival machines and multiply very quickly with eggs being laid within the first 24 to 48 hours after a female flea takes a blood meal on the host. Up to 50 eggs daily can be laid throughout the flea’s life span – potentially leading to a rapid explosion of the flea population. The majority of a flea’s life stages are in the environment and not found on the host.
Due to commonly used topical therapy in patients with CAD, most notably shampoo therapy, systemic flea control is the method preferred by many veterinary dermatologists. Molecules such as selamectin, spinosad and isoxazoline class drugs (fluralaner, sarolaner and afoxolaner) are useful in avoiding the compound being washed off towards the end of the treatment interval, which may result in loss of efficacy.

Staphylococci are normal commensals on the skin surface. However, when a primary disease, such as CAD, is present, the population can increase, lose diversity and cause a flare of the condition (Figure 8). Several studies have demonstrated, in both man and dogs, the skin microbiome changes in this instance. This state adds to the itch units of the given patient and needs to be addressed.
First of all, it is very important to correctly diagnose a bacterial infection. This is best done by cytology. A culture taken from the skin surface will almost always yield staphylococci, as they are usually present on the skin anyway. Culture and sensitivity testing is, therefore, best reserved for cases where cytology has shown rod-shaped organisms, to identify the species and their more unreliable sensitivity pattern, and for cases that fail to respond to an appropriate therapy (both in terms of the antibiotic chosen as well as the dose and dosing regimen) for an adequate length of time with good owner compliance to see if resistance may be an issue.
Many bacterial surface and superficial infections can be successfully treated with topical therapy alone. In the interest of antibiotic stewardship, this method should be pursued whenever possible; however, in some cases, systemic antibiotic are indicated for the acute phase.
Topical therapy, such as shampoos, wipes, sprays or mousses, can also be very useful for the long-term avoidance of relapses of bacterial pyoderma within the management programme for patients with CAD prone to this issue. Weekly routine shampoos – for example, with a chlorhexidine or chlorhexidine combination shampoo and possibly in conjunction with daily wiping, spraying or application of mousse preparations with antibacterial compounds – are very useful for this purpose. Each patient and owner will be different and respond better to certain combinations. Client education will result in much better compliance and is, therefore, a very important aspect of patient care.

Malassezia dermatitis (Figure 9) and otitis are probably among the most pruritic complications of dogs with CAD. Many patients are prone to yeast overgrowth, some breeds (for example, basset hounds, beagles and West Highland white terriers) more than others, and some individuals seem to favour yeast rather than bacteria.
Patients can also react with yeast overgrowth after antibiotic therapy. The same principles for diagnosis and therapy apply for bacterial overgrowth. Yeast overgrowth is also best diagnosed by cytology. Therapy can consist of topical preparations and, occasionally, systemic antifungal medication may be indicated.
Anyone who frequently washes his or her hands, and suffers from resulting dry skin, will confirm it can be very pruritic. Dry skin in dogs (Figure 10) leads to gaps in the lipid layer of the skin surface and, possibly, more leaky skin, which can enable allergens to penetrate the skin better. Patients with atopic dermatitis often suffer from dry skin. Moisturisers are the mainstay therapy used in the treatment of humans with this condition, and this is also very useful for our canine patients.
Medics have recognised in their human patients that stress is a factor not to be underestimated for many disease states. The mind-body connection is very strong and many different relaxation techniques are successfully used in human patients to improve their clinical signs in many diseases, including atopic dermatitis and asthma. It is, therefore, conceivable the same principle applies for our small animal patients. Moving home, losing a companion (human carer or other pet in the house), a new baby in the household or similar event all have an impact on our patients’ stress levels and may cause flare-ups of atopic dermatitis.
Confident pets will be better equipped to deal with changes in their life, just like in humans. Behavioural therapy, environmental enrichment and sprays and collars with pheromones and natural essential oils may be helpful in some patients to alleviate the stress and possibly influence the clinical signs due to atopic dermatitis.

Skin irritants are substances that cause slight inflammation or other discomfort to the skin, with no associated hypersensitivity reaction. As the irritation they can cause will be associated with itch units – just like other things discussed in this article – they can also contribute to the overall pruritus score and should be identified and avoided. Certain topical treatments, for example, can fall into this category. Owners often report their dogs’ clinical signs deteriorate after they have been on freshly cut grass, so this may be such an irritant.
Itching is transmitted by unmyelinated polymodal C fibres specific for this sensation. In human patients, heating the skin to 41°C relieves itching, but not pain, which is one of the facts in favour of specific nerve fibres transmitting pruritus versus pain. In contrast, owners of dogs with CAD often report an increase in the pruritus score during the summer months. This may be due to the heat itself, an increase in the levels of relevant allergens, conditions conducive for secondary infections or parasites or heat resulting in dry skin.
Humidity can have a negative or positive influence on pruritus. Low humidity can cause transepidermal water loss and lead to dry skin, with an increase in pruritus. However, high humidity favours mould growth, and in mould-allergic individuals, this can exacerbate the condition. Certain temperature/humidity constellations are favourable for the house dust mite and flea population growth, which can cause further itch units. It is also conceivable higher levels of humidity favour microbial growth on the skin in general, or certain strains of microorganisms in particular.
Although many of the aforementioned hypotheses have not been thoroughly examined and documented in the literature for our pet patients, some factors demonstrably play an important role – namely, secondary infections and parasites, and others are likely to be involved (for example, stress, humidity and dry skin).
Flare factors are contributing to the level of pruritus in patients affected with CAD to a large extent. It is, therefore, very important to identify and treat/rectify those factors as much as possible.
Successful control of those factors will make control of the underlying allergy far easier and, in mild cases, systemic antipruritic therapy may no longer be needed.