15 Aug 2023
Luca Ferasin DVM, PhD, CertVC, PGCert(HE), DipECVIM-CA(Cardiology), GPCert(B&PS), FRCVS and Heidi Ferasin BVSc, CertVC, MRCVS work through some of the clinical techniques for the investigation and interpretation of this feline finding.

Image: © Photocreo Bednarek / Adobe Stock
Cardiac auscultation is a fundamental part of a thorough clinical examination in all cats and the identification of individuals that may benefit from a medical or surgical intervention, or routine monitoring, often depends on a clinician’s ability to detect and interpret the presence of a heart murmur.

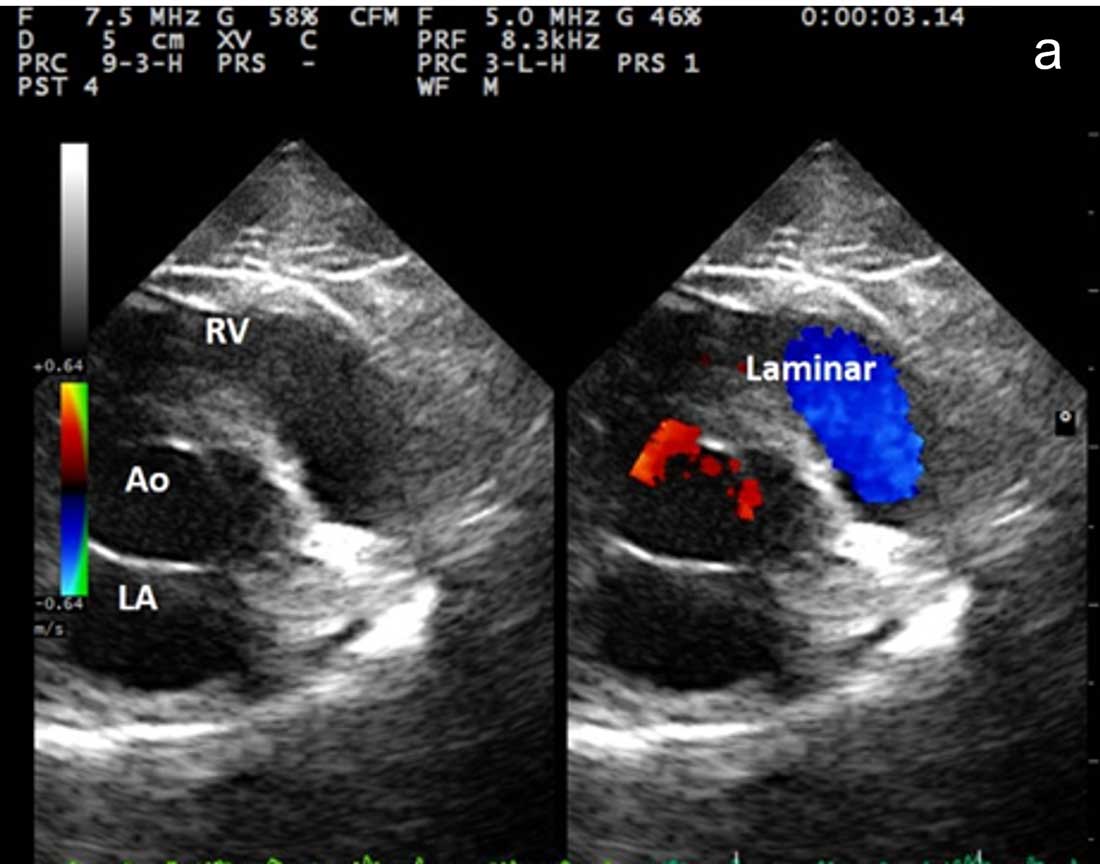
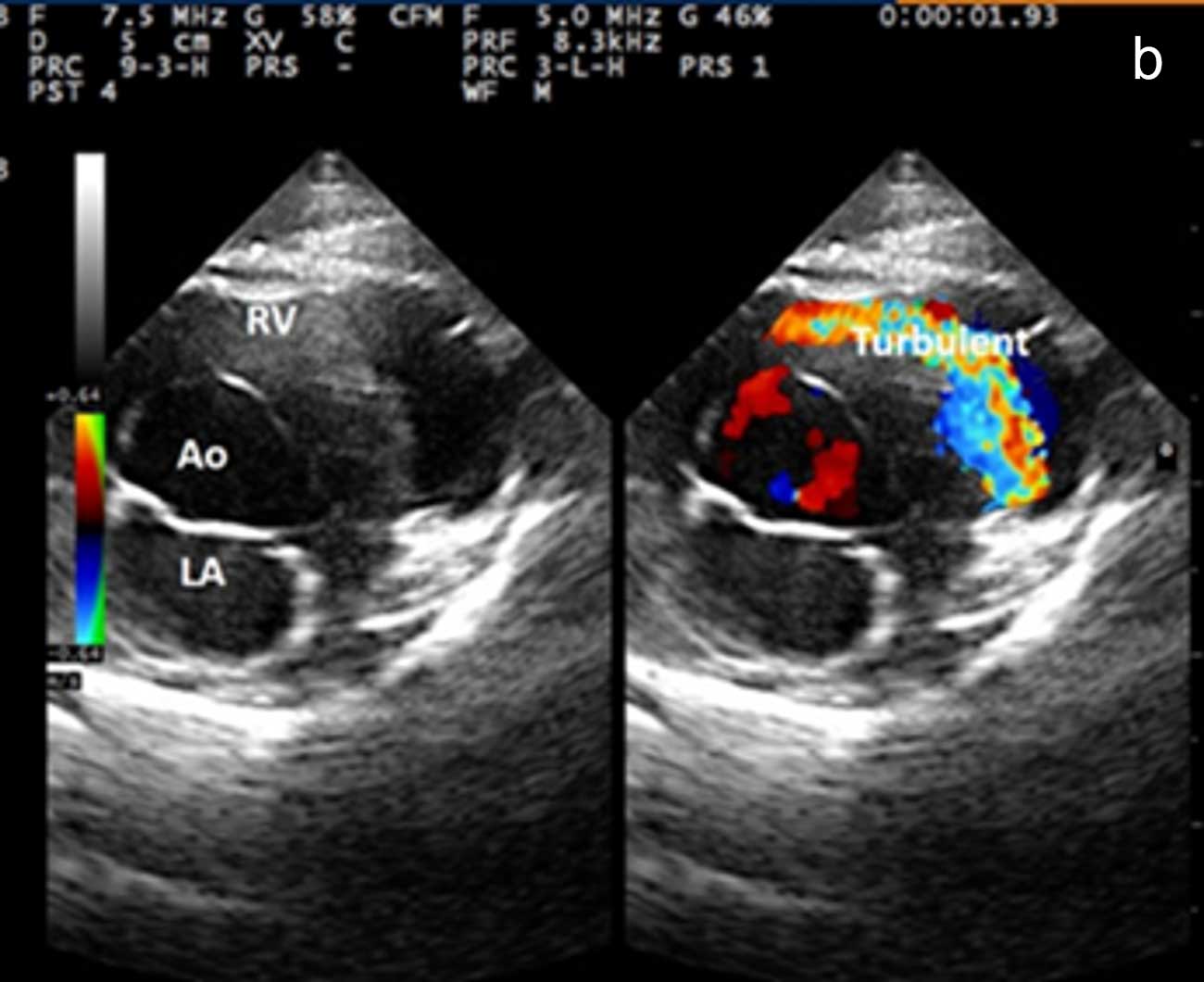
Heart murmurs are vibrations created by the blood when its flow changes from laminar to turbulent, producing a loud enough sound that can be heard with a stethoscope.
Heart murmurs are a relatively common finding in both young and adult cats. However, it should be noted that, in many cases, the presence of an audible murmur on cardiac auscultation in a cat does not necessarily imply the presence of a significant underlying cardiac disease.
Several studies have been published in the past to address the prevalence and clinical significance of heart murmurs in cats, but very few have looked into the exact origin of the blood flow turbulence responsible for this finding.
Therefore, it is important to adopt a different approach to the investigation and interpretation of heart murmurs in cats, to obtain the best results and provide an optimal standard of care in veterinary practice.
Thoracic auscultation has historically been considered as a safe, inexpensive and accurate means of diagnosis. However, in the current climate of both human and veterinary medicine, an increase in reliance on diagnostic imaging has decreased the emphasis on physical examination, leading to an erosion in physical exam skills, including cardiac auscultation.
Furthermore, it has been demonstrated that the auscultation skills of recent veterinary graduates are no better than final-year veterinary students, suggesting that cardiac auscultation is somewhat neglected in the current continuing development1.
Cardiac auscultation in cats is performed by placing the stethoscope head flat on the chest wall, being careful not to press it too hard on the point of contact to avoid the risk of evoking iatrogenic heart murmurs, which will be explained in an upcoming section of this article.
For auscultation in cats, the authors prefer to use infant or paediatric traditional stethoscopes, of which heads contain a diaphragm (the larger and flatter side of the chest piece) and a bell (the smaller, concave piece with a little hole in the middle).
The diaphragm of the stethoscope is typically used to hear normal to high-pitched sounds that can occur during the cardiac cycle, while the bell can be used to hear low-pitched sounds. Therefore, clinicians should always use both components of the chest piece to characterise abnormal heart sounds efficiently – especially heart murmurs.
A proper auscultation in cats should be performed in a quiet environment – ideally away from dogs or other cats – to allow the patient to be comfortable and relaxed, since changes in heart rate expected during periods of stress may alter the auscultatory findings.
It is also important to remember that approximately 20% of cats examined in veterinary practice purr during cardiac auscultation and this sound, dramatically amplified by the stethoscope, represents an important distraction. Indeed, significant auscultatory abnormalities, such as heart murmurs and gallop sounds (both of which are brief, low-frequency sounds, often of quite low intensity) can be masked by purring.
Various techniques have been proposed over the years to stop cats purring during thoracic auscultation; however, the most successful method is to perform auscultation in the proximity of a running tap, which can stop cats purring in 80% of cases. To obtain the best results, the cat should be held within 0.5m to 2m of a running faucet while performing heart auscultation (Figure 1)2.
When a heart murmur is detected, it is important to describe its timing (systolic/diastolic/continuous), intensity grade and location (point of maximal intensity; PMI).
The timing of heart murmurs in cats has been reported as systolic in 98.7% of cases, diastolic in 0.7% and continuous in 0.6% of cats with a heart murmur3.
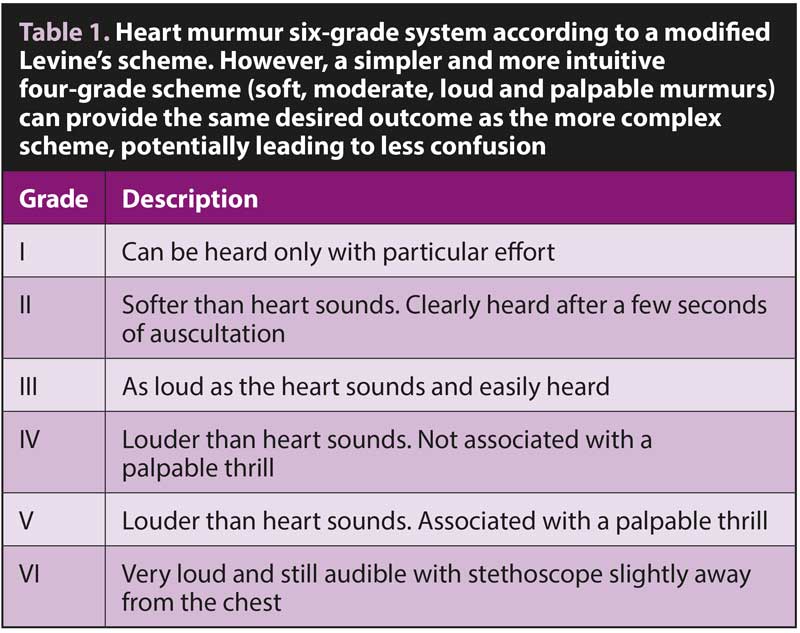
Traditionally, heart murmur intensity is classified according to a modified Levine system (Table 1); although, a simplified method describing murmurs as soft, moderate, loud and palpable (that is, discernible thrill) is perfectly acceptable4.
Based on this simplified system, the majority of cats display a soft murmur (56.7%), followed by moderate (28.7%), loud (12.6%) and palpable (2.1%). Furthermore, heart murmurs in cats often vary in intensity (dynamic heart murmurs). These types of murmurs can be detected in approximately 30% of cats and they are usually associated with a dynamic outflow obstruction3.
Veterinary textbooks often report four standard points for heart auscultation, which are referred to as aortic, pulmonary, mitral (on the left side of the chest) and tricuspid (right side of the chest). While these reference points may be useful and reliable in large animals, or large-breed dogs, the head of the stethoscope can easily cover multiple points in small animals, including cats.
Furthermore, most heart murmurs in cats are best heard at the level of the sternal or left or right parasternal areas, making the traditional standard points irrelevant. Therefore, the authors prefer to focus their auscultation on the sternal/parasternal areas.
The continuous murmur caused by a patent ductus arteriosus in cats is louder at the level of the left axilla; although, these cases are often accompanied by loud murmurs that can radiate to the left parasternal area. In the largest study of heart murmurs in cats, the PMI was described as sternal (or “both parasternal”) in 38.3% of cases, followed by left parasternal (37.2%), right parasternal (21.7%), left base (2%) and left apex (0.8%)3.
Heart murmurs in young kittens are mostly identified during physical examination at their first vaccination and can be associated with a congenital disease in approximately 40% of cases. The remaining cases of heart murmurs in this subgroup are associated with flow murmurs (60%), often called “innocent murmurs”.
In one of the authors’ studies looking at the prevalence of heart murmurs in 856 cats, the youngest kittens diagnosed with an acquired cardiac disease (hypertrophic cardiomyopathy [HCM] phenotype) were six months old and the echocardiographic changes were associated with suspected acute myocarditis, which was followed by a complete reverse cardiac remodelling (confirmed on repeat echocardiographic examination) after a few weeks and accompanied by complete disappearance of their heart murmur.
This echocardiographic observation is also referred to as transient myocardial thickening (TMT) or transient cardiac hypertrophy (TCH); although, it should be emphasised that TMT/TCH is not an aetiology per se, but purely an echocardiographic/morphological observation of a transient biological event reported both in cats and human patients due to various causes, such as myocarditis, diabetes, Takotsubo syndrome, reperfusion therapy in acute myocardial infarction, and so forth5,6.
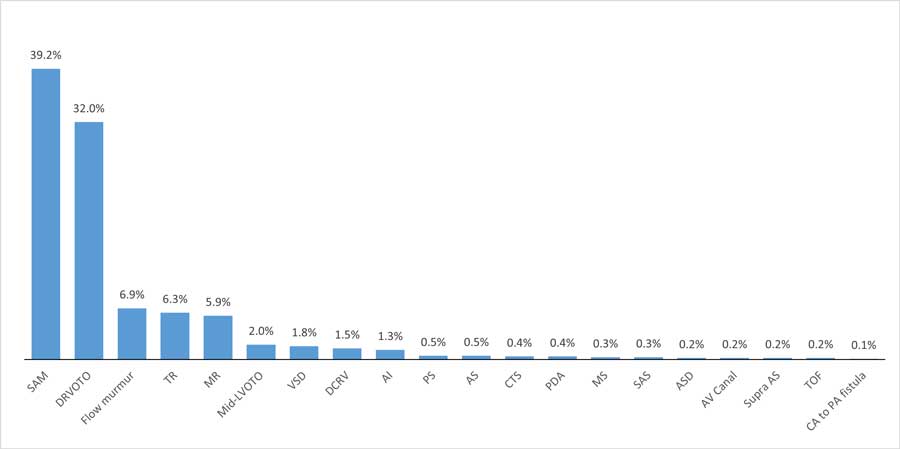
Dynamic left ventricular outflow obstruction secondary to systolic anterior motion of the mitral valve (SAM) is the most common cause of heart murmurs in cats, having been identified in approximately 40% of individuals. The second most common cause is another form of dynamic obstruction affecting the right ventricular outflow (dynamic right ventricular outflow tract obstruction; DRVOTO), observed in more than 30% of cats with a heart murmur.
Flow murmurs are diagnosed in approximately 6% of cats, where the origin of the blood flow turbulence is not detectable during colour flow Doppler echocardiographic examination.
Other causes of blood flow turbulence responsible for feline heart murmurs are outlined in Figure 2.
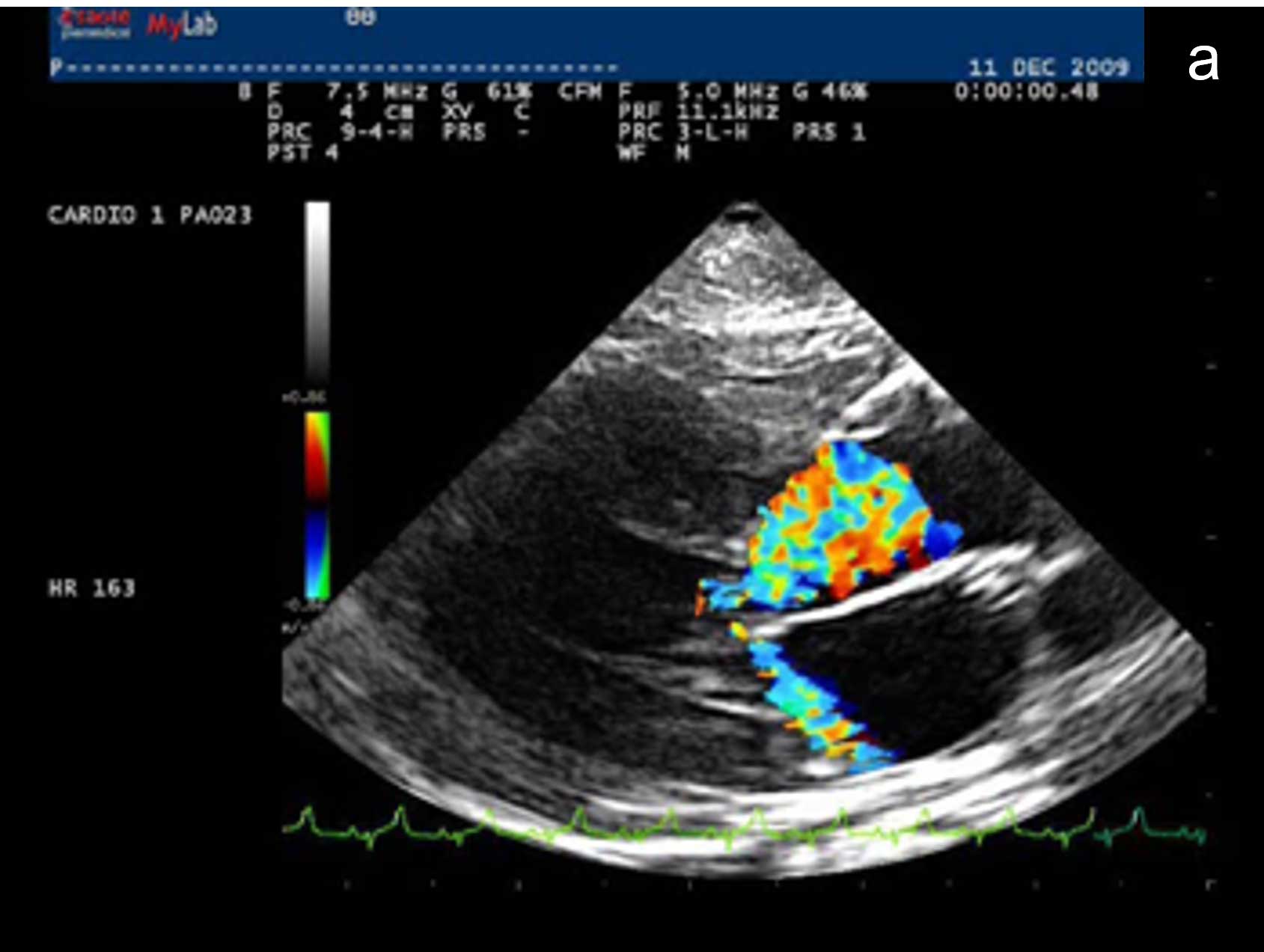
Although some clinicians confirm a diagnosis of SAM simply based on a systolic movement of the septal mitral valve leaflet toward the left ventricular outflow tract on 2D echocardiography, the authors believe that this criterion alone may lead to an overestimation of this phenomenon, and they advocate the confirmation of SAM based on concurrent detection of the following echocardiographic features:
An example of echocardiographic diagnosis of SAM in a cat is reported in Figure 3.
Although the mechanisms responsible for SAM in cats are not completely understood, it has been hypothesised that exuberant contraction of the left ventricle – as well as abnormal anatomy and arrangement of the mitral valve apparatus, including mitral valve leaflets, chordae tendineae and papillary muscles – may be contributing factors.
In human patients, SAM has historically been reported in association with HCM. The tendency to group these two conditions together has also persisted in small animal medicine. However, despite this common misconception, SAM is not pathognomonic for HCM, having been convincingly documented even in the absence of left ventricular hypertrophy in humans, dogs and cats. It has also been reported that some cats display echocardiographic evidence of SAM only during periods of what appeared to be sympathetic stimulation (such as stress or excitement), which is perhaps suggestive of a functional abnormality in these individuals influenced by loading conditions and exuberant myocardial contraction.
This sympathetic stimulation can be easily reproduced during the echocardiographic examination following a sudden increased loudness of the Doppler sound through the speakers of the ultrasound machine (provocative manoeuvre). However, some cats demonstrate SAM throughout the entire echocardiographic examination, regardless of perceived sympathetic stimulation, which is perhaps more suggestive of anatomical changes of the mitral valve apparatus and left ventricle7.
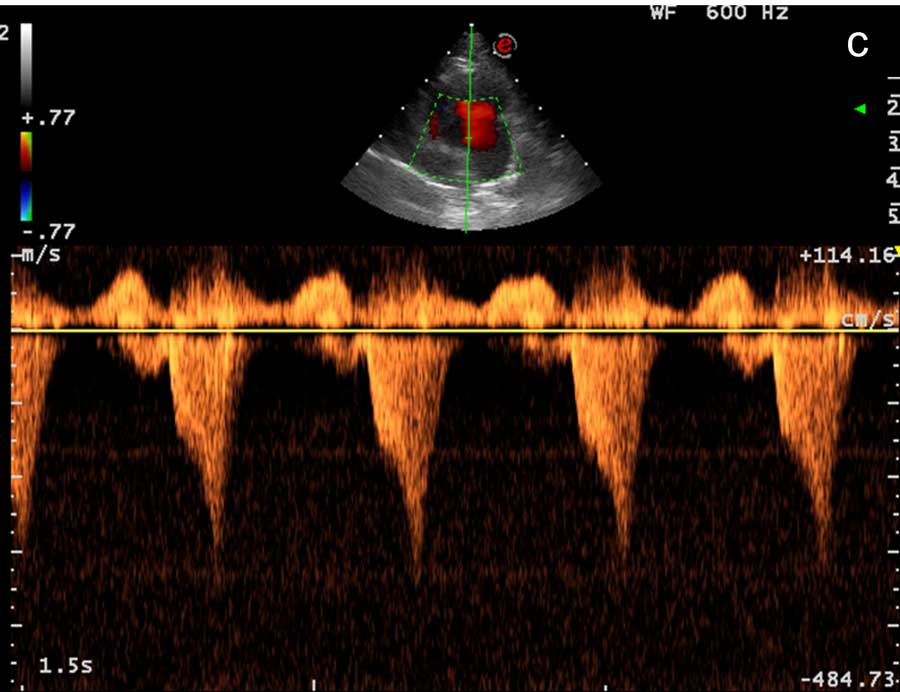
DRVOTO is a type of functional systolic murmur that has been identified in cats and believed to be due to a dynamic narrowing of the right ventricular (RV) outflow tract – especially in young and elderly subjects. The pathophysiology is poorly understood, but it seems to be associated with an exuberant contraction of the right ventricle, which tends to obliterate the right outflow tract in systole causing turbulence in the infundibular area.
It has been reported with higher prevalence in geriatric cats with anaemia, hypertension or hyperthyroidism, but it is also observed in apparently healthy cats.
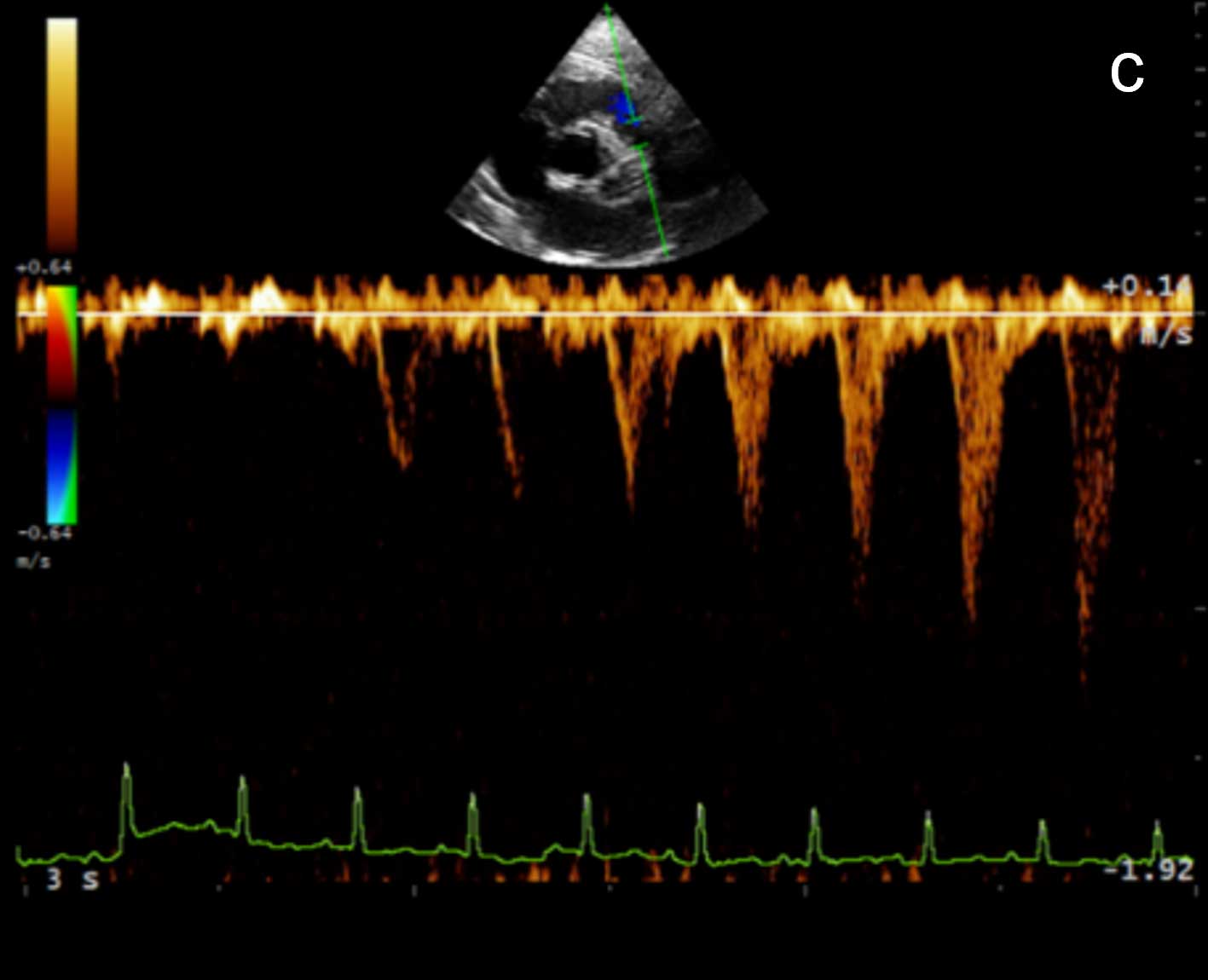
Diagnosis of DRVOTO is achieved by confirming a systolic colour Doppler aliasing in the right ventricle, just cranial to the tricuspid valve and extending into the RV outflow tract, associated with spectral dispersion and a scimitar-like appearance of the RV outflow profile on spectral Doppler study.
In the first report of DRVOTO in cats, heart murmurs were dynamic (varied in loudness) with changes in excitement level and heart rate. Furthermore, the velocity of the turbulent flow in the RV outflow tract consistently increased with increasing heart rate, while it diminished when the heart rate decreased, often returning to a normal laminar flow8.
However, this phenomenon was not observed in another study, suggesting that the dynamic obstruction may not necessarily occur secondary to an adrenergic response9.
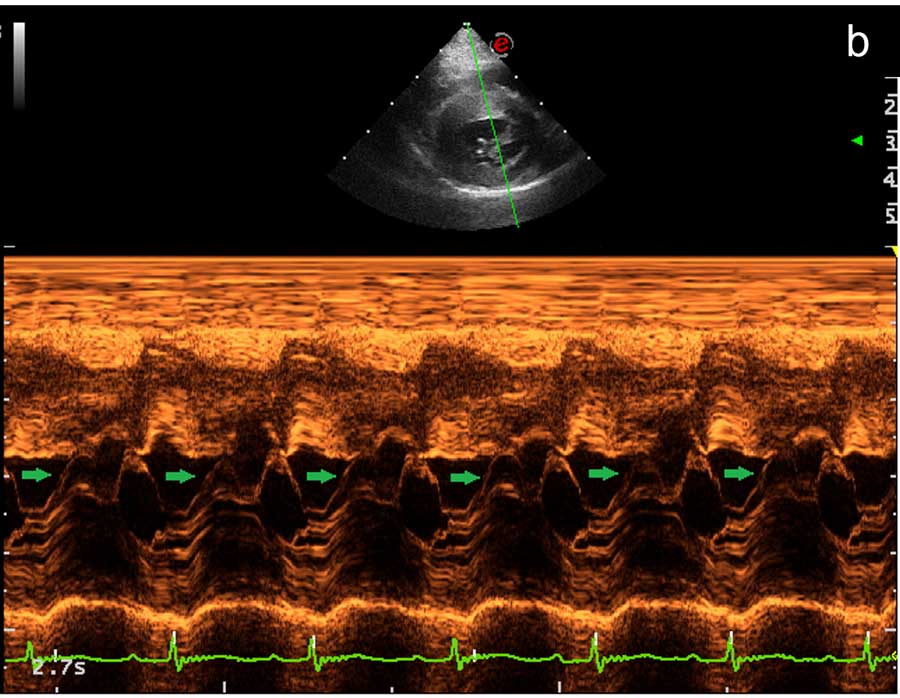
Inducible DRVOTO has also been reported as a blood flow turbulence obtained by applying a gentle pressure with the ultrasound transducer to the right parasternal area of the cat (provocative manoeuvre), inducing an iatrogenic dynamic outflow obstruction (Figure 4)9.
A gentle pressure with the stethoscope on the right parasternal region of the chest during cardiac auscultation in cats may induce an audible murmur, which subsequently disappears once this pressure is released, in analogy with the iatrogenic DRVOTO reported previously.
Results of a recently published study indicate that iatrogenic heart murmurs occur in apparently healthy cats, with an average prevalence of nearly 30%. The most plausible explanation of these inducible murmurs in cats is a DRVOTO.
The lack of association between heart rate and inducible murmurs in that study indicates that an increased adrenergic tone does not play a factor in the presence or absence of right-sided iatrogenic murmurs.
Increasing age and decreasing body condition scores were both identified as being associated with a higher chance of inducing a murmur. However, while increasing age was associated with a greater chance of producing an iatrogenic murmur, heart murmurs can also be iatrogenically induced in younger cats.
Therefore, veterinarians should always consider iatrogenic right-sided murmurs as a differential diagnosis when an audible soft, systolic murmur occurs when gentle pressure is applied to the right parasternal region in cats10.
More than 50% of cats with an audible heart murmur do not have any echocardiographic evidence of structural heart disease, suggesting most heart murmurs in cats are benign or may be potentially associated with a subclinical form of heart disease not detectable echocardiographically at the time of assessment.
Heart murmur characteristics (timing, intensity and location) can rarely discriminate between normal cats and cats with underlying cardiac disease, with the exception of loud and palpable murmurs inevitably associated with a significant heart disease.
However, since the majority of heart murmurs in cats appear to be systolic and mild-moderate in loudness, echocardiography, ideally performed by an experienced cardiologist, should always be considered following identification of a heart murmur on clinical examination in cats – especially when the patient does not present any clinical signs referable to a heart disease.
If an echocardiographic assessment is not feasible due to lack of adequate equipment (for example, Doppler capabilities), clinician’s expertise or financial constraints, measurement of cardiac biomarkers (for example, N-terminal prohormone of brain natriuretic peptide and cardiac troponin-I) can provide a useful screening test, since most haemodynamically significant heart murmurs are often accompanied by an increased level of these biomarkers7.