28 Sept 2015

Figures 11 to 13. Wound lavage system consists of a 1L bag of isotonic crystalloid, pressure sleeve (set to 300mmHg), a giving set and a 20 gauge hypodermic needle attached at the end of the giving set.
Dogs and cats are commonly presented to veterinary practices after traumatic incidents. These patients often suffer injuries to multiple body systems. As a result, it is important to assess the patient globally. This includes initial triage of patients, providing analgesia, thorough physical examination (including orthopaedic and neurological assessment), diagnostic investigations (such as blood tests and diagnostic imaging) and surgical treatment, if necessary, once the patient is stable. It is important to not plainly focus on obvious fractures and overlook other common injuries.
If there is an open fracture, it is important to promptly cover it with sterile bandage to minimise further contamination of the wound. Intravenous antibiotic should also be started at the earliest opportunity. Once the patient has been stabilised, wound debridement can start, either as a separate procedure or at the time of fracture repair. Articular and open fractures should be repaired at the earliest opportunity once the patient is stable. Fractures distal to the elbow and stifle could be temporarily stabilised with modified/Robert Jones bandage prior to surgical repair. Patients with fractures proximal to the elbow and stifle should be cage rested until definitive treatment. Alternatively, a spica splint could be used to temporarily stabilise proximal limb fracture.
Dogs and cats are commonly presented to veterinary practices after traumatic incidents.
Road traffic accidents, falls from height and being kicked by horses are some of the commonly seen trauma cases. These patients often suffer injuries to multiple body systems, including the head and neck, thorax and abdomen. Fractures of the limbs are not uncommon in these patients.
On initial presentation, each trauma patient should be assessed using the airway-breathing-circulation (A-B-C) triage guidelines.
Is the patient conscious and breathing? If the patient is not breathing, intubate and ventilate.
If the patient is breathing, oxygen supplementation may be required and this can be provided by means of an oxygen mask, oxygen tent/cage or nasal prongs.

Intravenous fluid therapy is often initiated, as many patients will be presented in hypovolaemic shock. This can manifest as tachycardia (or bradycardia in decompensating shock or in cats), poor peripheral pulse, cold extremities and pale mucous membrane with slow capillary refill time. Isotonic crystalloid (isotonic saline/0.9% NaCl and Hartmann’s solution/compound sodium lactate) is often the initial treatment of choice.
Hypertonic saline solution and colloids can also be used as supplementation. The commonly used fluid types and rates are listed in Table 1.
Once the initial triage is performed, it is important to provide patient analgesia. This will increase patient comfort and improve the ease of patient handling, as well as reducing the detrimental effect of pain on trauma patient, such as increased myocardial metabolic rate and oxygen consumption, predisposition to cardiac arrhythmia, reluctance of patient to move/walk/breathe and pain-related ileus.

Opioids and NSAIDs are often the first choices. It is important to establish the patient is not azotaemic before considering NSAIDs. Patients with pre-existing renal insufficiency, marked dehydration or that have urinary tract rupture may be azotaemic and the use of NSAIDs in these patients is cautioned against.
Other analgesic options include paracetamol, tramadol, lidocaine and ketamine. A multimodal approach is recommended to improve patient comfort and to reduce undesirable effects of individual medications. The doses of the commonly used medications are listed in Table 2.
After the initial A-B-C assessment, further patient assessment should be performed to assess any disabilities. A thorough physical, neurological and orthopaedic examination is required. Diagnostic investigations such as blood tests and diagnostic imaging are necessary.
After the initial triage and administration of analgesia, it is important to assess the patient globally and not become fixated on the obvious fracture/s.
Haematology, or at the very least, the PCV, is assessed for any evidence of anaemia, haemoconcentration, leukocytosis and to be documented as baseline. Serum biochemistry and electrolytes levels should be measured to establish a baseline as well as evaluating any evidence of azotaemia, concurrent elevated liver enzymes, electrolytes imbalance and reduced protein levels.
These parameters may be within the normal limits in acute situations and close, ongoing monitoring is recommended, especially if the patient’s recovery is taking longer than expected or if the patient is deteriorating.
Patients suffering severe trauma often have a prolonged recovery period and the blood profiles may need to be assessed regularly for the guidance of ongoing fluid therapy, the need of blood products, for early signs of systemic inflammatory response syndrome.


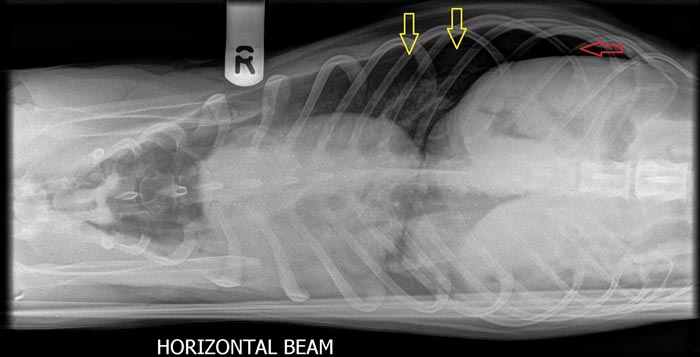
Patients may present with tachypnoea, but may also display increased respiratory effort. Although this can be commonly associated with pain, it is important to assess for thoracic injury. It has been reported up to 40% of cats5 and up to 79% of dogs3 with thoracic trauma do not have clinical signs of thoracic injury. Documentation of this is important as part of the global assessment of patient status as well as providing additional considerations for further general anaesthesia for interventional procedures, such as fracture repair.
In a distressed patient, it is advisable to provide oxygen supplementation, fluid therapy and analgesia prior to thoracic imaging. A general survey radiograph (for example, “catogram” or “dogogram”) of the whole body in sternal recumbency is useful to assess for severe pneumothorax or pleural effusion, which would warrant thoracocentesis prior to further investigation. Once the patient is stabilised, three-view thoracic radiographs should be taken to fully assess any thoracic injury.
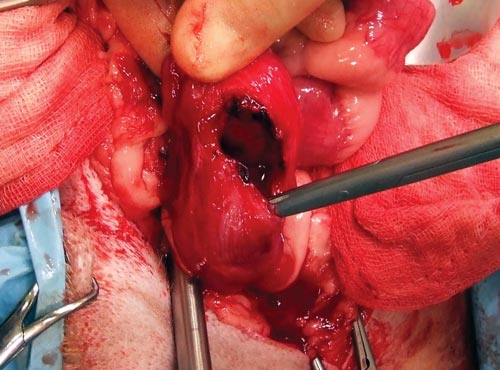
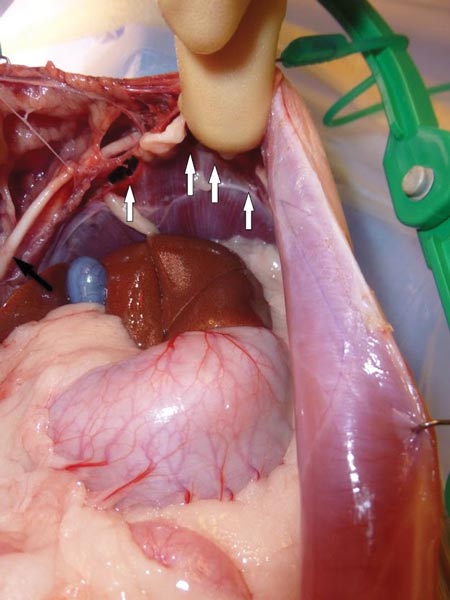
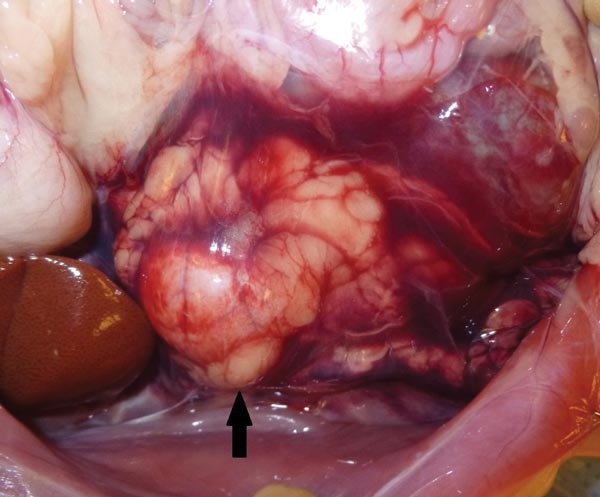
Patients can suffer from uroabdomen secondary to urinary bladder rupture (Figure 4) or haemoabdomen secondary to contusion/fracture of the abdominal organs, such as liver and spleen. Rupture of the abdominal wall or diaphragm can also be seen (Figures 5 and 6).
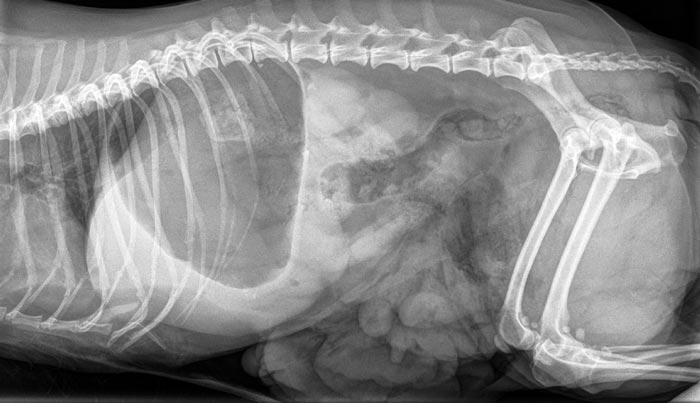

An abdominal ultrasound is useful to assess the abdomen for any evidence of free abdominal fluid. Abdominal radiographs can also be performed to assess for decrease or loss of serosal detail and the absence of certain abdominal organs, such as the bladder.
The presence of a urinary bladder silhouette does not preclude the possibility of a rupture. A positive contrast study of the urinary tract is useful in the diagnosis of urethral (Figure 7) or bladder rupture.
Fractures of the skeletal system are common in trauma patients. The femur and pelvis are the most commonly fractured bones in cats whereas radius/ulna and pelvis are the most common fractured bones in dogs7.

If there is an open fracture (Figure 8), a temporary, non-adhesive sterile bandage should be applied over the fracture site to minimise further contamination, especially from hospital-borne bacteria, while the patient is being assessed and stabilised.
A neurological exam should be performed whenever possible and this should include the mentation of the patient, cranial nerve function, any spinal pain, proprioception, withdrawal and spinal reflexes of the limbs.
It is often difficult to assess the proprioception of the fractured limb. In these cases, one should at least establish the presence of sensation with or without voluntary motor function on the affected limb.
It is important to note the presence of withdrawal and spinal reflexes do not equate to voluntary motor function and the presence of sensation. Withdrawal and spinal reflexes can be present as long as the local spinal segment is intact, despite the interruption of the spinal segment cranial to it.
It is also important to assess anal tone, perineal reflex and tail tone, especially if the hindlimbs and the lumbosacral area are affected. The reduced or absence of anal tone and perineal reflex indicates sacral spinal cord segment (S1 to S3) dysfunction. This can result in urinary and faecal incontinence. The prognosis of return of urinary continence is good if the anal tone and perineal reflex is present at the time of presentation. Cats that remain urinary-incontinent for a month after the injury generally do not regain urinary continence8.
A fracture is classified as open if there is full thickness skin wound/laceration overlaying the fracture site, however small the wound is (Figures 8 to 10).


Frequently, the fractured bones are not visible through the skin wound. Despite this, one has to assume the fractured bone may have penetrated the skin before reducing back within the skin. As such the bone has been exposed to the external environment and has been contaminated. Classification of open fractures is listed in Table 3.

These fractures should be thoroughly flushed with copious volumes of sterile isotonic saline (0.9% sodium chloride) or Hartmann’s solution.
A pressure of 7psi to 15psi is ideal to flush out gross contamination without driving the contamination into the soft tissue. A one-litre bag of saline/Hartmann’s in a pressure sleeve (cuff pressure 300 mmHg), attached to 16 to 22 gauge hypodermic needles is an ideal way to achieve this10 (Figures 11 to 13).



The size of the needle does not result in significant difference in pressure generated. A 35ml syringe attached to an 18 gauge or 19 gauge needle has been widely recommended previously to achieve this psi, but studies have shown this achieves too high pressure, up to 40psi. This may cause trauma to the wound.
Another common practice is to use a plastic saline bottle (500ml and one litre) with a needle punctured through the cap. Regardless of the size of the bottles or the needles and the fluid level, this does not generate the desired pressure of 7psi to 8psi10.
After thorough flushing, necrotic tissue and debris can be debrided further mechanically (bandages), surgically or enzymatically.

After debridement, if soft tissue envelops/coverage is not immediately established, a bandage with primary sterile layer should be applied. The sterile primary layer should ideally be absorbent and non-adhesive, such as Allevyn (Figure 14).
When the patient is stable and the wound is fully debrided, a definitive fracture repair can follow. In certain cases, some degree of surgical debridement is required in addition to the bandage/enzymatic debridement, either during the same procedure for fracture repair or as a separate procedure.

Established evidence shows prompt administration of broad-spectrum IV antibiotic reduces the infection rate in open fractures. The recommended first-line antibiotics are listed in Table 4. A bacteriology swab should be taken post-debridement as guidance for future antimicrobial therapy.
If the fracture is closed and there is no other wound requiring antimicrobial treatment, antibiotics are generally not given until the immediate perioperative period for the surgical repair.
Most fractures can be managed temporarily by the application of supportive bandage (modified/Robert Jones bandage; Figures 15 to 17) or cage-resting the patient until definitive fracture repair can be achieved. Carefully applied splint could also be useful for the temporary stabilisation (Figure 18). Supportive bandages can temporarily immobilise the fractures, minimise further soft tissue disruption from the fractured bones and improve patient comfort.




The supportive bandage is only useful to immobilise and protect the fracture sites distal to the elbows and stifles. To effectively immobilise the joint, the supportive bandage has to span the limb from the foot to one joint proximal to the fracture. This is difficult to achieve in fractures that involve or are proximal to the stifles and elbows. Not only will it not be able to span the joint proximal to the fracture (hips and shoulders), it is also prone to slipping, due to the conical shape of the limb with the bulky part proximally. As a result, the supportive bandage will fail to immobilise the fracture, and also act as additional weight at the extremity of the limb, increasing the pivoting effect at the fracture site.
Most fractures can be delayed for definitive repair for a few days; however, if the fracture involves articular surfaces or is open, the fracture repair is somewhat more exigent. These fractures should be repaired or debrided as soon as the patient is stable for anaesthesia.