30 Jan 2024
In this edition of his Diagnostic Dilemmas series, Francesco Cian recalls the case of a nine-year-old golden retriever presented to the referring veterinarian for the sudden enlargement of peripheral lymph nodes.
Francesco Cian
Job Title
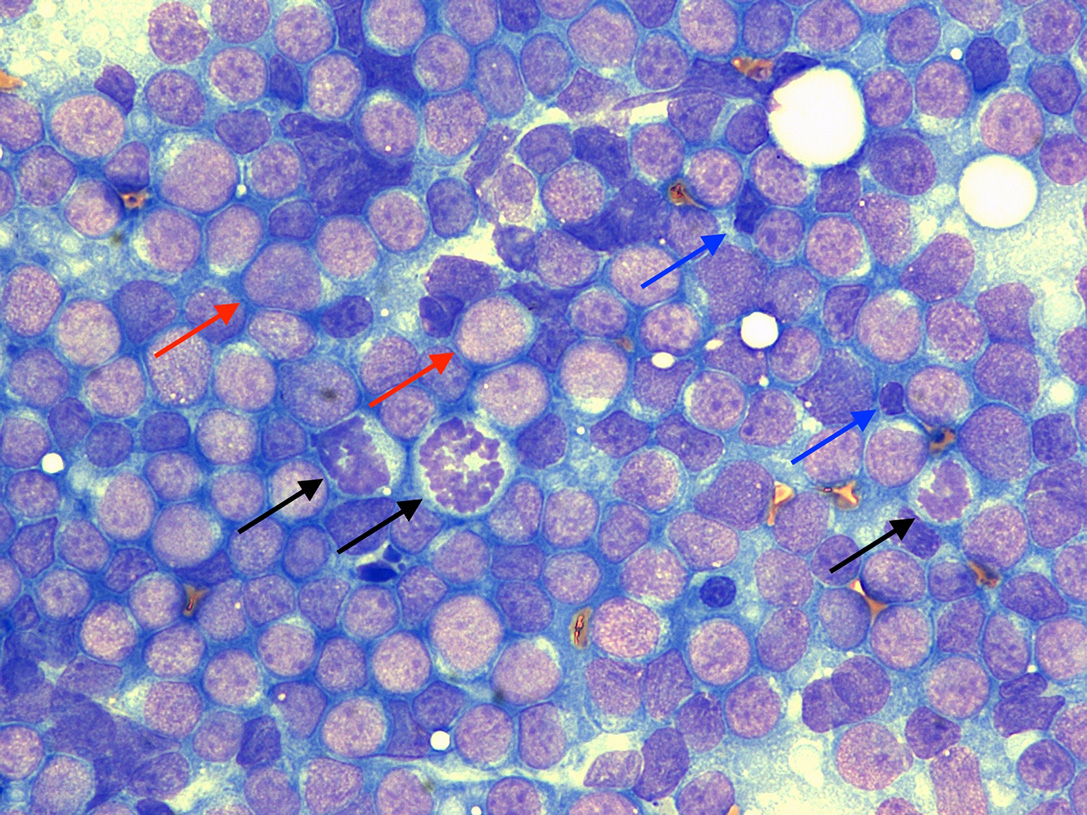
Figure 1. Aspirate from an enlarged prescapular lymph node in a dog, Wright-Giemsa 50×.
A nine-year-old female, neutered golden retriever presented to the referring veterinarian for the sudden enlargement of peripheral lymph nodes – in particular, prescapular ones.
Initial differential diagnoses included lymphoma, metastatic neoplasia, lymphoid hyperplasia and lymphadenitis. Fine-needle aspirates from all enlarged lymph nodes were collected and submitted to an external laboratory for analysis.
As per Figure 1, the aspirates from all lymph nodes were highly cellular, with adequate preservation. The background was slightly basophilic with rounded, light to dark blue cytoplasmic fragments – also named lymphoglandular bodies – and rare red blood cells.
A main population of mainly large lymphoid cells (red arrows) was present, which had scant basophilic cytoplasm, defined borders and a large, eccentric nucleus (more than 2.5 red blood cells), with stippled chromatin and small nucleoli sometimes visible. Numerous mitotic figures were seen (black arrows). Rare small lymphocytes (blue arrows) and scattered other leukocytes were noted.
A diagnosis of large cell lymphoma was determined.
Full clinical staging was performed and did not reveal involvement of other organs; haematology was unremarkable. The patient was classified as stage three (generalised lymph node enlargement with no involvement of liver/spleen/bone marrow).
Flow cytometry was performed on fresh lymph node samples, and the neoplastic population was positive to CD79a and CD21 – both of which are B-cell markers, confirming the diagnosis of a diffuse large B-cell lymphoma (DLBCL), according to the World Health Organization (WHO) classification for neoplastic diseases of the lymphoid tissues.
The dog received a 25-week CHOP protocol (University of Wisconsin-Madison) and achieved complete remission on the third week of treatment. It remained in remission all along the chemotherapy protocol and for the following five months. Eleven months after its diagnosis, the lymphoma relapsed and a rescue protocol was then started.
The four anatomic forms of lymphoma seen in dogs include multicentric, mediastinal, alimentary and extranodal. The multicentric form accounts for more than 80% of lymphomas and is characterised by generalised lymphadenopathy, with or without hepatomegaly, splenomegaly and bone marrow involvement. Clinical signs are often non-specific and include weight loss, anorexia and lethargy.
According to the WHO classification, different morphological subtypes of lymphoma exist, which should be identified, as they may have a different clinical behaviour and response to therapy. This lymphoma was identified as DLBCL and represents the most common subtype in dogs; it often has a multicentric clinical presentation.
The prognostic factors most consistently identified for high-grade canine multicentric lymphoma include WHO morphological subtype, immunophenotype (T-cell versus B-cell), WHO clinical stage/substage, and steroid pre-treatment.
Many reports have confirmed that dogs with high-grade B-cell disease have significantly longer remission and survival durations than dogs with high-grade T-cell lymphomas. In particular, canine DLBCL has a variable clinical course, with median survival times reported to be 191 to greater than 300 days with multi-agent chemotherapy. On the other hand, dogs with indolent subtypes may live years, often even without therapeutic intervention.
Cytology is often sufficient to emit a diagnosis of lymphoma, and is characterised in most cases by a predominance of a monomorphic population of lymphoid cells (usually more than 50%) that lack the pleomorphism commonly seen in reactive processes.
Further tests – including flow cytometry, PCR for antigen receptor rearrangements, immunocytochemistry and/or histopathology (often coupled with immunohistochemistry) – may be considered to confirm and/or to refine the diagnosis.
Lymphoma is not one disease, but refers to a heterogeneous group of haematological malignancies largely divided into aggressive and indolent forms.
These are characterised by very different clinical behaviour and prognosis, and treatment may need to be approached in different ways.
The aetiology of lymphoma is complex, involving both genetic and environmental factors. Certain breeds are over-represented, suggesting a genetic risk component.
Interestingly, studies have identified geographic differences in lymphoma prevalence and subtype distribution, even among high-risk breeds; for example, the golden retriever is over-represented among dogs with lymphoma in the US, but this does not seem to occur in Europe.
nvironmental risk factors may explain the different breed risks observed between American and European studies, but the possibility also exists of differing genetic predisposition to lymphoma between American and European golden retriever breed lineages.