1 Sept 2021
Fay Cameron BSc, BVSc(Hons), MRCVS recounts the case of a Russian toy terrier presenting with medial patella luxation and right hindlimb lameness.
Fay Cameron
Job Title
Arya, a two-year-old entire female Russian toy terrier, presented with a grade 2/4 right medial patella luxation and progressively worsening right hindlimb lameness.
Abnormal limb alignment is known to play a significant role in medial patella luxation and CT has been shown to have high precision in the assessment of femoral alignment in the frontal plane1,2.
Assessment of femoral torsion or anteversion angle (AA) from radiographs can only be made through complex trigonometry of perfectly positioned orthogonal views of the femur3‑5. Whereas assessment with CT is relatively straightforward, repeatable, requires far less time positioning the patient and avoids having to repeat exposures to acquire perfectly positioned views.
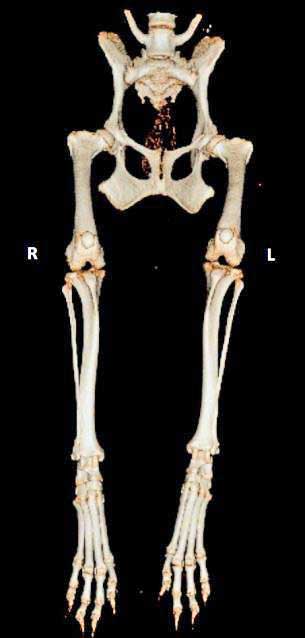
To determine if significant limb malalignment existed, a CT scan of Arya’s hindlimbs was performed. This revealed a femoral retroversion after making measurements of femoral torsion from the CT images (Figure 1).
Femoral AA typically ranges from 10° to 40° in normal dogs without patella luxation, with the accepted normal being 25°. Any femoral AA lower than the normal range may be contributing to the patella luxation, as the patella will not naturally sit in the trochlear groove due to abnormal alignment2,6-11.
Arya’s AA measured -10° and given this was so abnormal, it was considered to be significantly contributing to quadriceps malalignment and so correction was likely necessary to resolve patella luxation. Standard surgical correction alone (medial release, lateral imbrication, tibial crest transposition and sulcoplasty) could have potentially been unsuccessful and resulted in reluxation of the patella post-surgery.
The frequency of patella reluxation after standard corrective surgery is normally around 8%12. Femoral varus or anatomic lateral distal femoral angle was also measured and this was normal. There was also no significant tibial malalignment.
CT data was used to create a 3D virtual model of the right femur in computer-aided design software. A transverse femoral osteotomy with torsional correction of 35° was modelled (aiming for a normal value of 25°), and a patient-specific osteotomy and reduction guide system designed (Vet 3D, Bill Oxley MA, VetMB, DSAS[Orth], MRCVS, Coventry; Figure 2).
These guides, along with 3D prints of the femur before and after the planned correction, were 3D-printed in biocompatible, autoclavable plastic. Evidence exists in both the human and veterinary literature that patient-specific surgical guide systems can improve osteotomy accuracy and reduce surgical time. This may be particularly important in smaller patients13,14.
Prior to surgery, Arya as premedicated with 5µg/kg dexmedetomidine and 0.3mg/kg morphine via IM injection – 4mg/kg propofol was administered IV for induction and anaesthesia was maintained on a combination of isoflurane, oxygen and nitrous oxide. A standard lateral approach was made to expose the distal femur, and the drill guide was fixed in position with 1.34mm bicortical negative end threaded pins.

The osteotomy guide was created in such a way that it was perfectly contoured to the distal aspect of the femur and could only fit in place one way. The osteotomy was made using an oscillating saw in the position and orientation directed by the guide. Once complete, the cutting guide was removed and a reduction guide was placed over the previously placed pins. This held the osteotomy segments reduced, with the planned torsional correction, while a seven-hole 2mm locking compression plate was applied laterally (Figure 3).
The pins and reduction guide were then removed. Subsequently the patella was running in the groove through extension and flexion, and no additional procedures (for example, sulcoplasty, tibial crest transposition, lateral imbrication or medial release) were required. The lateral approach was closed routinely using 2m polydioxanone, 2m poliglycaprone 25 and 2m nylon.
Arya was strictly cage rested for six weeks. At follow-up, she walked without lameness and on clinical exam the patella remained in position throughout a full range of motion. Radiographs were taken at this stage, which confirmed healing of the osteotomy was progressing well (Figure 4). Arya was then able to gradually resume normal activity.
The author would like to acknowledge Patrick A Ridge BVSc, CertVR, CertSAS, MRCVS and Bill Oxley MA, VetMB, DSAS(Orth), MRCVS.


