20 Aug 2018
David Beeston explains how some of his most rewarding veterinary experiences have happened during out-of-hours shifts. Includes video content.
David Beeston
Job Title
Image: Svetlana Barchan / Adobe Stock.
On call work can be gruelling, unsociable and, all in all, undesirable. However, over the past year, some of my most rewarding experiences have happened during the widely dreaded out-of-hours work.
Realising (at the time of writing) I have just ceased to be a “new graduate”, I thought it would be nice to take time to reflect on some of the lessons I’ve learned from taking the telephones for the night.
My first story took place in autumn 2017. Picture this: after a long day of work, I am the late vet on site and my final consult of the day is booked in – “cat won’t stop vomiting”. After a quick check of the cat’s history, I can see it hasn’t been seen since 2013, and the final notes are regarding a postoperative check following a cat spay.
The female cat, which will henceforth be known as El Diablo, had chased my colleague around the room in what can only be accurately described as the whirlwind cartoon character, The Tasmanian Devil.
Prepared, or so I thought, I called the client in and began taking a history. El Diablo had managed to find her way into her owner’s lunch and had stolen a white chocolate cookie. After chowing down on what must have been a delicious mid-afternoon snack, the cat had proceeded to vomit multiple times and became even more distressed than usual.
El Diablo had been disturbingly quiet in her carrier, so I cautiously opened the lid and allowed her time to acclimatise to the horrifying environment of my consult room.
Lightly petting the cat in an attempt to assess the health and safety risk, I was pleasantly surprised to find her quite amenable to a good chin scratch. I managed to assess the cat’s teeth and mucous membrane colour – I even had a quick look under her tongue and moved to cardiothoracic auscultation.
“This is going so well”, I thought. “Let’s move on to the abdomen.” In a flying fury of claws, teeth and faeces, El Diablo had decided enough was enough. With my not-so-ninja-like reflexes, I managed to simultaneously open the carrier door and back away, hoping she’d take the bait. She did.
The owner, looking pale and apologetic, explained El Diablo hadn’t been to the vets because the fiasco that happened four years ago had been so scarring (in more ways than one), they thought it inappropriate to inflict her wrath on unsuspecting vets for routine health checks.
With a limited history, and even more limited physical exam, my mind was racing towards the potential of either a dietary-induced gastrointestinal upset or foreign body. I advised the client I would like to take x-rays, given the high frequency of vomiting, but the owner opted for a jab of maropitant and a wait-and-see approach. Easier said than done, a crush cage allowed an SC injection of maropitant and I returned the cat to her willing owner’s arms, who I instructed to telephone me if any further vomiting occurred.
The next morning at 3am, the telephone rang: “Leonard Brothers Emergency Service, Dave speaking, how can I help?”
El Diablo had vomited again. Being a new graduate with very limited experience, I thought this required immediate attention, so I telephoned one of the practice nurses to meet me at the clinic. Having now been informed El Diablo’s “tapas menu” was not only the cookie, but potentially an array of office supplies – including sticky tack and elastic bands – I gave her a nice jab of medetomidine, butorphanol and ketamine (DTK), and soon “sleeping beauty” was flat enough to x-ray.
To my surprise – bar a small amount of gaseous distension in the colon – the x-rays were relatively unremarkable. A jab of maropitant and atipamezole later, El Diablo was staring at me through her cage, plotting her revenge. I told her owners to keep an eye on her and telephone me if any further vomiting occurred – we’d repeat the x-rays and see if any change had occurred. The owner was happy with the plan and, first thing in the morning, I got my more senior colleagues to examine the x-rays, who agreed no obvious surgical lesion was present.
Soon enough, El Diablo’s owners had telephoned to say the cat still wasn’t right, but hadn’t vomited again. She wasn’t keen to eat and they were particularly worried. Back to the crush cage – and a jab of DTK later, we repeated the x-rays. No real change. So, I performed a pneumocolon x-ray to check the distension was definitely in the colon, which it was, and subsequently gave El Diablo a treat involving some warm water and chlorhexidine gluconate. With some quite “explosive” results, I figured El Diablo had just become a bit “backed up”, so I sent her home with the instructions to sit tight and let me know if any changes occurred.
The next day, one of El Diablo’s owners telephoned and said: “Really sorry to bother you, but she’s just vomited a small amount of bile up, should I be concerned?” Going with my gut, I decided we needed to look inside El Diablo, due to the progressively chronic history. Assisted and supervised by a senior colleague, we got El Diablo prepped for surgery and I performed my first exploratory laparotomy. True enough, a concoction of rubber bands and sticky tack could be seen in the distal colon.
After milking out what I imagine Stretch Armstrong’s faeces to look like, and getting one of the nurses to grab and pull it out of El Diablo’s rear, I checked the rest of her abdomen. Spotting a solitary mid-jejunal hard lump, I nervously proceeded to do my first enterotomy and exteriorised a 1.5cm object.
“I think this cat has eaten a nut,” I said to my supervisor. After closing up, I telephoned the owners and explained my findings, asking them to come down in a few hours once El Diablo had recovered.
Talking through my generic discharge instructions and getting ready to say goodbye to my trusted companion/dragon, the client had an epiphany and said: “Oh no, it must have been one of those white chocolate and macadamia nut cookies from Subway.”
The moral of this story? Not every foreign body will be visible on x-ray, and history is probably the most important part of any case.
At my practice, the vets receive OOH telephone calls directly. While this has made me much more proficient in obtaining capsule histories and triaging over the telephone, it does come with some downsides. Despite the adrenaline rush when I hear that horrendously annoying default ringtone, it is not always deserved, and for every true emergency, I probably have 10 to 15 non-emergency telephone calls.
Ranging from 4am telephone calls about cats – “which would normally be outside hunting at this hour” – to 11pm panics about a newly discovered lump, I like to think I remain professional and courteous at all times. Albeit frustrating, owners often don’t know what constitutes an emergency, and sometimes all they want is a bit of advice and reassurance.
Of course, this isn’t limited to OOH, as I often have consults involving the conversation: “Oh, we get worried about blood in human poo, but it can just be a normal presentation of large bowel diarrhoea in our small furry companions.” It can be difficult to assess over the telephone, however, so I will always offer to see an animal in need.
The lesson I’ve learned about taking telephone calls is take every concern seriously and you won’t miss a thing. Write something off immediately and you’ll regret it that 1 time out of 100 where there was more to the story.
Due to some rearranging of weekends, I had quite the stretch of on call shifts this summer. I can’t complain, as it was entirely self-inflicted, but after my fourth weekend in 7 weeks (compared to the usual 1 in 10 weekends), I can honestly say I was knackered. The following tale comes from the first of those four weekends, and involved a lovely female Italian spinone named Pickles, which belonged to fellow on call nurse Bev.
We’ve been very lucky with the weather this year, but, unfortunately, it has meant an increase in the exercise-induced cases I’ve seen. After an incredibly hot Sunday, Bev telephoned me to say she had just been out on a walk and Pickles was struggling to breathe. Listening to the breathing over the phone, I could hear quite the roar, and I advised Bev to get straight to the practice and try to keep Pickles cool on the way.
Each vet at our practice appears to have certain cases he or she attracts. For one of my colleagues it is cats involved in road traffic collisions; for another, it is always status epilepticus. For me, it is respiratory emergencies. Having quite a keen interest in emergency and critical care and the use of point-of-care ultrasound, my practice will vouch for the fact I get the scanner out for most of my emergencies. As soon as I got to the practice that Sunday afternoon, my mind went into autopilot and I got ready to see Pickles – not sure what state she would be in on arrival.
Thankfully, Pickles came walking in with only a mildly increased respiratory effort; she had clearly settled once out of the heat. I proceeded to triage her and noticed an increased upper respiratory tract noise on tracheal auscultation – otherwise, her lungs were clear and she appeared stable. The mild dyspnoea was on inspiration, but the roar had subsided. I placed a catheter and gave Pickles a nice slosh of butorphanol, and let her calm down.
A thoracic-focused assessment with sonography for trauma was unremarkable, and my top differential – given signalment and the initial presentation of an inspiratory obstructive pattern with stridor – was laryngeal paralysis. It is never easy dealing with a colleague’s pet, especially when you’ve not managed a case with a similar presentation.
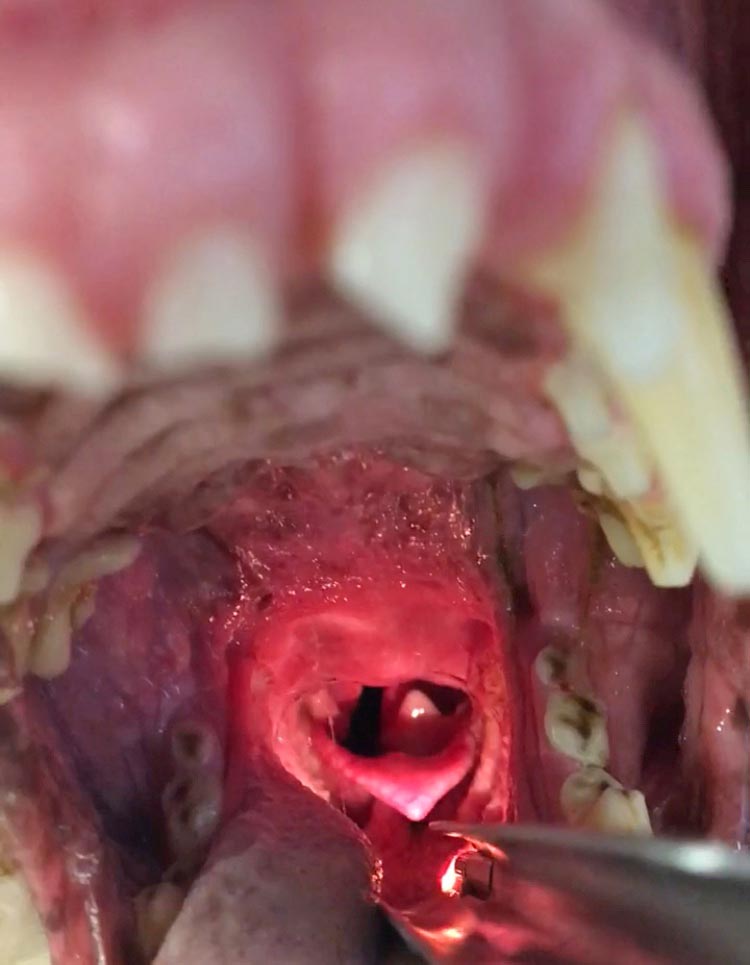
Over the past 10 months, I’ve found random snippets of information will pop into my head at the right time – presumably because they’re buried deep down somewhere, waiting to be retrieved. I knew to confirm my diagnosis I would need to visualise Pickles’ larynx under sedation. I gave Pickles a light dose of alfaxalone (0.25mg/kg) and got to visualising her airway (Figure 1).
As far as I could tell, Pickles’ larynx was not normal and a bilateral laryngeal paralysis appeared to exist.
Pickles went on to be referred to Northwest Veterinary Specialists and has subsequently had surgery to repair her defective arytenoids. She has recovered remarkably and I’m proud to say I had a part to play in her journey. Pickles taught me I should be confident in my abilities. It is easy to panic, especially in emergency situations, but having algorithms in your head to rely on can really take some of the excess thinking noise out of the picture.
I can’t believe how quickly this year is going, and although the safety blanket of calling myself a new graduate will soon be gone, I am proud of what I’ve been achieving. By meeting up with my fellow graduates, it is incredible to see how far we’ve come. Only 12 months ago I hadn’t even done my solo vaccination consult, and now I’m somewhat confidently dealing with emergencies.
The stories I’ve heard from my university friends are incredible and I think we often forget how far we’ve come. When you’re having a rough day, doubting your knowledge and wondering if this is all worth it, just remember where you started. Remember how much work you’ve put in to getting to where you are and that you are being trusted by clients to deal with their beloved animals, and realise how much of an honour that really is.
To my fellow recent graduates, and those entering the profession over the coming weeks, we are still in the very early days of our careers, and have the opportunity to grow in many directions.
Be proud of what you’re doing, because you deserve to be.