9 Jan 2017
James Elliott assesses methods of discovery for this condition and suggests treatments.
James Elliott
Job Title
Figure 1. Nasal discharge is a common presenting sign in dogs with nasal tumours, though it is also present in other nasal diseases.
Canine sinonasal tumours are rare in dogs, representing approximately one per cent of all neoplasms. However, in referral oncology practice this is a tumour dealt with frequently, and appropriate diagnostics are required to achieve a robust diagnosis and advise clients on appropriate treatment plans.

Although dogs as young as one year old have been reported with these tumours, generally it is a disease of older, medium-to-large breed dolichocephalic dogs. Conflicting data exists as to whether tobacco smoke and indoor exposure to fossil fuel combustion products increases the risk of this tumour type.
Carcinomas represent approximately two out of three of these tumours, with sarcomas representing around one out of three.
Of course, a few other weird and wonderful diagnoses, such as melanoma and mast cell tumour, are reported. Lymphoma, while being the most common nasal tumour in cats, is relatively rare in dogs. Some studies have shown overexpression of the tumour suppressor gene p53 and cyclooxygenase-2. These may potentially become part of our prognostic database and/or therapeutic targets in the future.
Unfortunately, various histological sub-types and tumour grades exist within the broad classification of carcinoma and sarcoma, which makes meaningful retrospective analysis of nasal tumour cases difficult.
Unfortunately, nasal tumours share many of the same historical and clinical examination findings as many other causes of nasal cavity disease, such as inflammatory rhinitis, fungal rhinitis and foreign bodies. This can make definitive diagnosis difficult and means we must rely heavily on additional diagnostic procedures and tests to reach a final diagnosis.
The most common clinical signs include nasal discharge (serous to mucopurulent; Figure 1), epistaxis, stridor, stertor, sneezing and facial deformity. Although lymph node metastasis does occur in a small proportion of cases, it would be extremely rare for this to be detected before clinical signs related to nasal disease became problematic and the focus of the investigation. Enlarged regional lymph nodes, if present, most likely reflect reactive hyperplasia. However, obviously cytological analysis is imperative to rule out the few cases with regional metastatic disease.
Some findings may help to differentiate the underlying cause of the clinical signs. Dogs with mycotic rhinitis (such as aspergillosis) may have profuse mucopurulent discharge that is often bilateral in the later stages, they often exhibit nasal or facial pain and a characteristic sign is depigmentation of the nasal planum beneath the discharging nostril(s).
Dogs with nasal tumours can occasionally have major discharge (through secondary bacterial infection or epistaxis), but this tends to be less profuse and rarely exhibits overt facial pain, and usually any discharge would be unilateral (at least initially).
Dogs with facial distortion almost invariably have cancer, although other causes are possible, including aspergillosis, while those with nasal foreign bodies often have an initially acute presentation with paroxysmal sneezing, facial irritation and agitation.
Canines should have their mouth closed and a piece of cotton wool placed at each nostril while they are breathing to assess airflow. Tumours are more likely to cause obstruction of airflow due to the presence of a soft tissue mass in the nasal cavity, while fungal plaques destroy much of the bony content of the nasal cavity and good airflow often remains, unless significant secretions cause obstructions.
The length of the clinical history is an important factor to take into consideration. Dogs with fungal rhinitis can have a protracted history of many months and/or some of the aforementioned signs. The average survival time of dogs with nasal tumours without treatment is three months, so a history exceeding this without significant progression of clinical signs or morbidity makes a tumour less likely, although not impossible.
All of the differential diagnoses that result in the classical signs of nasal cavity disease in the dog require an appropriate workup for diagnosis and treatment. It is well-accepted primary bacterial rhinitis almost never happens in dogs, so cases that initially/repeatedly respond to antibiotics with or without NSAIDs/steroid-based therapy should be evaluated for underlying pathology as they will invariably recur.
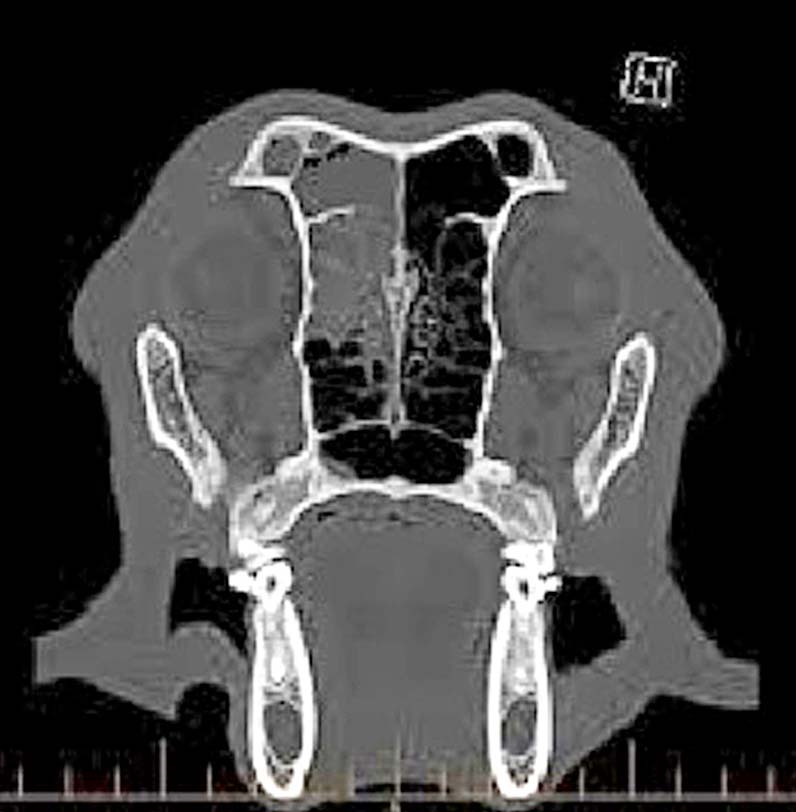
Radiography has been largely superseded in some practices and most referral hospitals by advanced imaging modalities, such as CT (Figure 2) and MRI. However, radiography remains the mainstay of initial nasal disease workup for most practitioners and is a great diagnostic tool.
Radiographic features of neoplasia include presence of a soft tissue mass, ipsilateral turbinate loss, surrounding bony invasion and soft tissue/fluid opacity in the ipsilateral frontal sinus. The most useful view to assess the nasal cavity is the intraoral dorsoventral view of the nasal cavity with the plate placed in the dog’s mouth and the beam directed from above.
Even with its inherent problems compared to CT/MRI, such as superimposition, the sensitivity of radiography is comparable to CT for detecting major airway abnormalities in dogs with nasal tumours, when the tumours are sufficiently advanced to cause clinical signs.
Imaging should always be undertaken prior to biopsy to visualise appropriate areas to biopsy and because heavy bleeding frequently occurs, which can distort images taken post-biopsy and make them hard or impossible to interpret.
If the area to biopsy is large and obvious on imaging, a blind biopsy via the nares can be obtained with forceps. This is cheaper, quicker and easier and, generally, bigger samples can be taken for histopathology – and culture if infectious rhinitis is suspected. The length of the biopsy instrument must be measured against the dog’s nose to avoid breaching the cribriform plate. Otherwise, biopsy via rhinoscopy is an option and fungal plaques can be visualised if this is the primary differential.
If a tumour is suspected clinically, with imaging support, nasal flushes can be performed to attain material for histology; however, if the cribriform plate is not intact (and, indeed, even if it is) then forced flushing can cause further damage and result in potentially catastrophic neurological signs. It is rare one must resort to surgical rhinotomy to attain sufficient material for diagnosis.
Although histological diagnosis (carcinoma versus sarcoma) has no effect on treatment recommendations at present, it is still advisable to perform histology to definitively diagnose a tumour prior to long and expensive therapies. This will also ensure a rare histological diagnosis, such as lymphoma, that may warrant different treatment and a different prognosis is not missed.
Routine staging of all tumour-bearing patients should include assessment of the primary tumour and its location and invasiveness.
The regional lymph nodes, along with the thorax and abdomen, should be surveyed to detect metastatic disease. This could include three-view, inflated thoracic radiographs and an abdominal ultrasound. If a CT scan is performed, this can be continued to include the thorax and abdomen once a mass is seen on head CT.
However, metastatic disease is extremely rare at presentation, so the cost of these additional procedures has to be discussed with the owners. Generally, fewer than 10 per cent of nasal tumour patients have evidence of metastatic disease at first presentation and clinical experience suggests this figure may still be an overestimate.
It may be more important to fine-needle aspirate both of the mandibular/regional lymph nodes, particularly in the case of carcinomas, as nodal metastases at presentation definitely occurs. Nodal metastasis has been shown to be a negative prognostic indicator in some studies and may affect treatment choice or aggressivity.
Several staging systems are available for nasal tumours, depending on the size, position and invasiveness, as seen with diagnostic imaging, and, for some tumours, stage is highly predictive of outcome. Some studies have shown the more locally extensive lesions are associated with a poorer prognosis, which seems logical. However, some have shown no convincing correlation between nasal tumour stage and survival/outcome.
Assessment is hampered by the variable numbers of dogs in each stage “group” in different studies, which makes accurate comparisons and conclusions difficult. It seems reasonable to assume dogs with very extensive primary disease, extensive breaching of the cribriform plate and tumour extension into the cranial vault, metastatic disease and severe facial deformity will have a poorer long-term outlook. More conservative approaches may be appropriate for this subset of patients.
CT scan and other imaging modalities are still important to aid in diagnosis, assess disease extent and guide biopsy accrual. CT is extremely advantageous for radiotherapy planning that allows avoidance of the critical structures surrounding the tumour mass, particularly the eyes and brain.
Surgery, radiotherapy and chemotherapy have all been assessed in the treatment of canine sinonasal tumours with varying degrees of success. The largest study looking at untreated dogs (no surgery, chemotherapy or radiation) showed an average survival of 95 days. However, some dogs may do better than this.
Surgery has been assessed extensively in the treatment of nasal tumours and it is accepted it does not play a major role in their treatment at present.
In various studies, surgery did not provide a survival advantage compared to dogs that had no treatment, and also did not provide an advantage to dogs that had surgical debulking performed prior to radiotherapy – compared to dogs that had radiotherapy alone. This is also a high-morbidity procedure and, therefore, cannot be recommended with no obvious patient benefits.
One report shows dogs had protracted survivals when they underwent surgical nasal exenteration after radiotherapy. However, many of these dogs developed chronic and severe side effects, such as bone necrosis, so it is considered by many oncologists to be unacceptable.

Radiotherapy (megavoltage) is considered the standard of care for dogs with nasal tumours. This can be given in two different ways:
This is probably the modality that has been the least satisfactorily studied. Attempts have been made to use drugs such as cisplatin, 5-fluorouracil and cyclophosphamide, biodegradable cisplatin-containing implant, low-dose carboplatin and gemcitabine as radio-sensitizers, and others with limited success.
One Australian study discussed using alternating doses of carboplatin and doxorubicin as a sole treatment when dogs could not receive the standard of care (radiation) and documented good tumour responses in some patients with some impressive results. However, only a small number of dogs were evaluated. This certainly warrants further study and perhaps combination with standard radiation protocols. Metronomic chemotherapy (cyclophosphamide/NSAIDs) may provide some palliative effects in cases where standard treatment options are denied.
Dogs may be treated with antibiotics (to treat secondary bacterial infection) and NSAIDs (for anti-inflammatory, analgesia and for any possible anti-tumour effects) alone. Some unpublished data suggests this may give survivals of around six months.
Other treatments that have been minimally evaluated include photodynamic therapy, increasing radiotherapy dose and giving “booster-doses” at the beginning of the radiation protocol. However, none has been particularly successful in attaining better outcomes at this time.
Intensity-modulated radiotherapy and helical tomotherapy are treatment modalities that may result in less dose to nearby sensitive structures and become more widely used in the future in an attempt to attain better survivals for veterinary patients. Re-irradiation of the nose, when the tumour recurs after the first course, has been reported with some impressive results, but can cause some difficult adverse effects to the eye and bone.
Dogs with typical signs of nasal disease should be evaluated with at least diagnostic imaging at an early stage to avoid missing nasal neoplasia. This will enable earlier treatment and, hopefully, improve prognosis for the individual patient.
Radiotherapy is the standard of care and is tolerated well by dogs. However, treatment is palliative and almost all dogs are euthanised due to local disease progression at a later date.