30 Jun 2021
Stuart Carmichael BVMS, MVM, DSAO, FRCVS begins this two-part article by discussing ways of making better use of clinical findings to improve vigilance of this issue.
Stuart Carmichael
Job Title
Image: © kintarapong / Adobe Stock
Diagnosis of OA is widely regarded as being straightforward in dogs. It often relies on obtaining a suspicious history in addition to recognising a combination of classical clinical signs – including limping, stiffness and difficulty rising or jumping – plus joint swelling, pain on manipulation and crepitus within a joint1.
Vigilance for OA exists in certain breeds and in older dogs due to the known higher prevalence within these groups.
Clinical diagnosis can be confirmed by using imaging to recognise osteophyte production and bone changes in established joint disease.
So, what is the problem?
If we look at the present level of recorded diagnoses versus the incidence of the disease in the population, a 75% discrepancy exists (Zoetis data). Why is this?
Are we really failing to recognise the disease in so many animals, or are we simply failing to take time to look for it?
Could another reason be that we do make a diagnosis, but then ignore it – and as a result fail to record it or initiate any treatment? Could this be because our threshold to initiate OA management is set far too high? And is this in part driven by the belief that we feel we cannot really make an impact on the clinical outcome or progress of the disease?
I have pinpointed four areas where we fall down:
The majority of these are failures to make better use of our clinical findings rather than failing to recognise the disease.
Diagnosis of OA in its early stages represents a challenge, as the cardinal signs are likely not well developed.
Dogs with early disease may show occasional bouts of lameness without any stiffness, crepitus or swelling, all of which are more apparent with progression. In addition, signs of early osteophyte proliferation may be subtle and easily missed or dismissed on images.
Acknowledging that OA is both present and a problem in younger dogs can be an issue of attitude. Having the conversation with an unsuspecting owner about the significance of the disease may be something that is avoided. This is combined with a general reluctance to intervene or use any medication in these young animals unless signs are very obvious.
A failure also exists to associate causal pathologies in younger animals with the presence of OA. As a result, hip dysplasia; elbow dysplasia, patella luxation and cruciate disease, when recognised, should have a simultaneous diagnosis of OA. Although this may be well‑understood, it is not often recorded – and sadly also not acted on as a result.

Many patients are diagnosed generically as having OA without any further attempt to understand fully how the disease is affecting the joint.
OA is a dynamic and progressive problem, and produces very different pathologies and clinical problems in early disease compared to late disease2.
Staging attempts to recognise how advanced the disease is. Management can then be based on targeting the problems related to the stage.
Often a generic diagnosis results in formulaic attempts at management that pay no attention to actual and specific problems present. Therefore, by not diagnosing exactly how the disease is causing its clinical problem, we are missing the chance for more creative and effective management.
We often perform a clinical appraisal of a joint to make a diagnosis, rather than to determine details that let us fully understand the problem and better inform our choice of management.
We are also guilty of some misconceptions about the disease and for using isolated features to conclude a more serious problem, rather than basing this on a full appraisal.
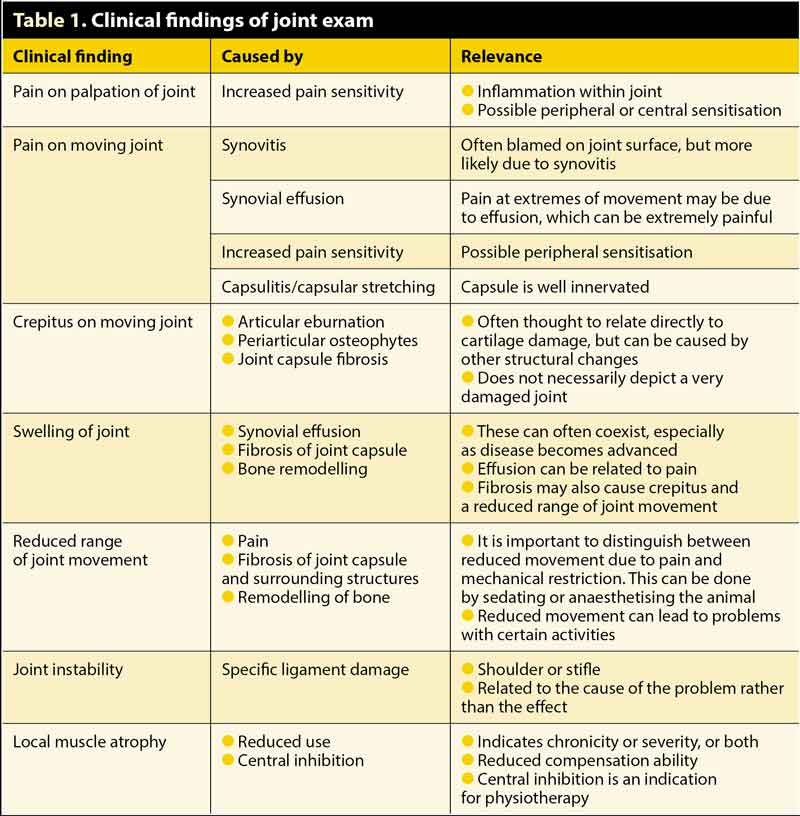
Pain is a common finding, often causing lameness. But do we consider why the joint is painful at diagnosis? Pain can be demonstrated by pressing the joint and surrounding tissues or by moving the joint. Pain on pressure is usually a worrying sign, especially if a marked response occurs, and could imply sensitisation.
Pain on movement is often thought to be due to damaged joint surfaces, but instead it is often due to a degree of synovitis, joint effusion and stretching of the joint capsule.
Crepitus is a common classical finding and often used as a marker of severity, but what is crepitus and what causes it? Most clinicians will conclude it is the result of cartilage loss at the articular surface, but it is just as likely to be a result of periarticular osteophytes or capsular fibrosis, both of which may imply a different prognosis (Table 1).
Many diagnoses of OA may be dismissed as of no consequence. This means the diagnosis is overlooked and not recorded. This leads to confusion with ongoing case management and an overall reduction in the number of cases recorded as having OA.
In older dogs, signs of OA can be dismissed as “ageing” and incorrectly accepted as a normal finding that does not require management. Often focus is on other problems or comorbidities that are deemed more serious, and so OA management is neglected.
We are also reluctant to both acknowledge the presence of the disease and its significance in younger dogs. We often fail to introduce comprehensive management at this stage, preferring to “wait until the pet really needs it”. This is really missing the point of the problem and making eventual management efforts much more difficult.
Small breeds with OA are similarly dismissed with the mistaken belief that OA does not cause the same problems as in larger breeds. The smaller breed may not present with the obvious mechanical signs that the larger dogs show, but the painful consequences are the same and may lead to more subtle presentations, much like cats with OA.
Another anatomical area where established OA is often overlooked or dismissed is when it is found in the distal limb area affecting the foot. Pathology is often found in multiple interphalangeal and metacarpal/metatarsal phalangeal joints, especially in older animals. Our tendency is to concentrate our management efforts on the major joints and ignore these smaller joints as less important.
Given how debilitating and painful OA is in the human foot and hand, I think this whole area requires review.
Often owners do not relate lameness to pain and OA. Carrying out “mobility surveys” can increase the awareness of the problem and, therefore, identify more animals that will benefit from earlier management.
The argument that these animals can cope with their joint problem does not really hold up against current evidence. Measures can be implemented that can have a profound effect on the problem.
Identification and focus on recognising early disease in higher-risk patients would also hugely increase the numbers of animals being managed for OA. We know certain groups of patients will have a higher likelihood of having pathology due to other problems that they have.
Therefore, target:
Having owners of “at risk” individuals complete an assessment using clinical metrology instruments (CMIs), which are now widely available (Liverpool OA in Dogs, Canine Brief Pain Inventory or Helsinki Pain Index)3-5 is not only a proactive way of identifying potential problems, but also actively involves the owners in the process, which is vital for compliance in management schemes.
“Practice makes perfect” is a common saying – and it is certainly true with OA assessment.
The more frequently assessments are conducted, the more routine and informative they become. This applies to the whole OA management team. Training RVNs to clinically assess OA patients better widens the skill set and allows monitoring via nurse clinics.
Lameness assessment and confirmation is an important clinical feature in many OA cases, yet a proper lameness examination is often not carried out during veterinary assessment. As a result, many clinicians have low confidence and perhaps low ability to perform a lameness examination.
Lameness assessment is made easier if the pet owner can present a short video clip taken on his or her mobile phone before or at the time of consultation. This whole area has been highlighted in remote consultations during COVID‑19 restrictions, but is equally valid in a face-to-face consultation. Owners receive instructions detailing how to take these clips to allow proper assessment. The clip can be viewed at leisure in the clinic at normal speed or in slow motion, making a gait abnormality much easier to appreciate.
Video clips of animals performing certain activities the owner is concerned about in his or her home environment can add valuable information.
Work on clinical assessment skills in each joint for various clinical features. Understand both their significance and how they relate to the disease of the joint (Table 1), and the resultant clinical impact. Use these as a trigger for different management strategies.
Earlier use of ancillary aids, as part of a more aggressive approach to identifying OA in joints, may involve sedation of animals to check joint movement while, at the same time, enabling imaging and arthrocentesis.
In particular, learn how early OA appears in standard imaging views. This will lead to increased positive confirmation of diagnosis and more information about the joint or joints affected, and more confidence in recommending management. It also helps to eliminate other possible causes of the clinical signs.
Synoviocentesis can also be carried out on sedated animals. This will relieve acute problems related to effusion and analysis will eliminate the possibility of an inflammatory joint, as well as providing additional information about the intra-articular environment.
How can you establish that OA really is impacting on a patient’s quality of life? And how can you persuade the owner that this is the case? We need to use a more objective assessment system that the client can easily understand.
Also, how do you establish that management is making more difference over time?
We do little at present to evaluate this. This requires agreed milestones and measures that can monitor both the clinical problem and the pathological advancement of the disease in affected joints.
Repeated clinical assessments, performed regularly with the results recorded in a way that can be used to judge progression, will achieve this. In addition, this information will display trends over time that can confirm actual improvement.
In practical terms, this means putting together a planned assessment schedule for individual patients and combining CMIs3-5 with other specific clinical measures, such as results of clinical veterinary assessment, goniometric measurements from joints and mobility information1.
Completing a detailed clinical assessment of an arthritic patient yields a more detailed understanding of the clinical and pathological problem, and can encourage more creative and effective intervention. Repeated assessments will develop understanding of the “travel” of the disease and encourage longer-term management.
Changing our attitude to OA as a disease would make the biggest impact in improving our level of diagnosis and improving our success in implementing longer-term management programmes. Simply deciding that OA is a disease that needs to be recognised early and managed, and having more belief in our efforts at management, will make a very significant difference to affected animals. So: