4 Apr 2016
Alessandro Conte reports on an eight-year-old male boxer that presented with a history of progressive forelimb lameness of eight weeks’ duration, in the latest in the Case Notes series.
Alessandro Conte
Job Title
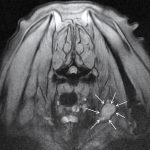
Figure 2. Transverse multiple echo recombined gradient echo MRI image of the caudal cervical region and the axillae. The tumour can be clearly seen affecting the left brachial plexus (arrows).
An eight-year-old male boxer is presented to you with a history of progressive forelimb lameness of eight weeks’ duration.
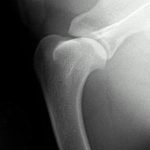
There was no history of any trauma. On examination, the dog exhibits a 6 out of 10 left forelimb lameness. Discomfort is evident on manipulation of the left shoulder and obvious spinatus muscle atrophy can be appreciated. Radiographs of the shoulder are obtained, but are unremarkable (Figure 1).
What is the primary differential diagnosis in this case and are there any other investigations you could consider?
In an older dog with significant forelimb lameness, apparent shoulder pain and an absence of a convincing orthopaedic cause for the problem, a peripheral nerve sheath tumour (PNST) involving the brachial plexus should be suspected.
These tumours are thought to develop from Schwann cells or local fibroblasts and can cause severe pain and lameness. They have low rate of metastasis, but have a strong tendency to invade adjacent neural tissues. The progressive growth of the tumour may result in invasion of the spinal canal and subsequent development of neurological deficits in other limbs.
PNSTs usually have an insidious onset of signs and can be difficult to distinguish from other causes of lameness, especially in the early stages of the disease. Typical clinical signs associated with a PNST can include:
If a PNST is suspected, radiography can be useful to exclude other orthopaedic causes of lameness, but this does not allow detailed assessment of regional soft tissues. Therefore, advanced imaging, such as MRI or contrast enhanced CT, should be considered.

Electromyography can be useful to demonstrate denervation within affected muscle groups; however, this is somewhat non-specific as similar findings can be seen with other neuropathies and certain myopathies. Myelography is rarely helpful unless the PNST has invaded the neural canal. Ultrasound can be effective in detecting PNST, but is highly operator-dependent and often needs to be supported by other imaging investigations, such as CT and MRI. Ultrasound-guided fine-needle aspiration of PNSTs have been described; however, non-diagnostic samples, false positives and false negatives are not uncommon.
Management options for PNST are limited. Palliative medical treatment can be attempted; however, many dogs fail to respond well. Local resection of the tumour is rarely possible and, in most cases, a forequarter amputation is recommended. The entire brachial plexus should be removed, with nerves transected as proximally as possible. In some cases, a foraminotomy or hemilaminectomy is also performed to excise the proximal portion of the spinal nerve as close to the spinal cord as possible.
Despite aggressive surgery, local recurrence in remaining neural tissue is common; however, many dogs can lead a good quality of life for several months. Owner satisfaction following amputation is generally very good. The dog in this case underwent a forequarter amputation. The owners reported it was doing well six months following surgery, although no further follow-up was available.