19 Sept 2023
Francesco Cian details the case of a six-year-old German shepherd dog presented for the presence of small bilateral corneal opacity and pigmentation in the ventro-lateral limbus of both eyes.
Francesco Cian
Job Title
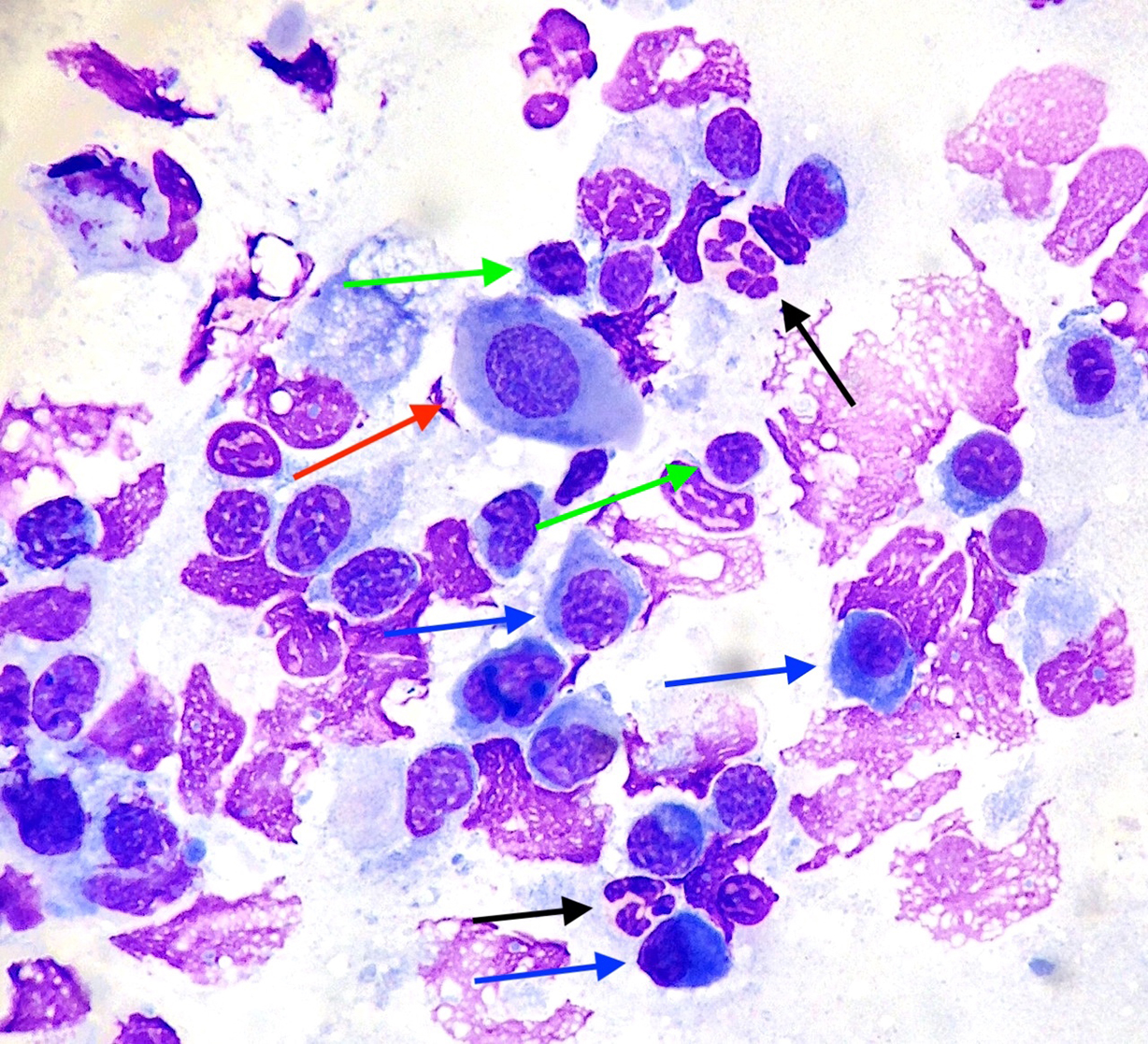
Figure 1. Cornea of a dog, Wright-Giemsa 50×.
A six-year-old male neutered German shepherd dog presented to the referring veterinarian for the presence of small bilateral corneal opacity and pigmentation in the ventro-lateral limbus of both eyes. The lesions did not appear to be painful. Clinical examination was otherwise unremarkable. Cytobrush sampling from these corneal lesions was performed and submitted to an external laboratory for analysis.
The sample contains numerous nucleated cells with variable preservation. The background is clear with variable amounts of cellular debris. A main population of plasma cells (blue arrows) is present, with a typical round cell appearance, deeply basophilic cytoplasm, perinuclear clear halo and eccentric nuclei. These are admixed with small lymphocytes (green arrows) characterised by a scant basophilic cytoplasmic rim and small, dark round nuclei.
Scattered segmented neutrophils (black arrows) and rare large polygonal epithelial cells, likely conjunctival/corneal in origin (red arrow), are also noted and do not show signs of atypia.
Lymphoplasmacytic inflammation, compatible with chronic superficial keratitis.
Chronic superficial keratitis (CSK), also known as pannus, is a bilateral, progressive and likely immune-mediated disorder of the canine cornea. It is characterised by raised, corneal pigmentation, vascularisation and hazy opacification, typically arising from the lateral limbus.
In a large percentage of cases, the third eyelid is concurrently affected and appears swollen and hyperaemic (termed plasmoma, atypical pannus or nictitans plasmacytic conjunctivitis).
This condition occurs more frequently in young adult German shepherd dogs, but can also be observed in other canine breeds. It is considered progressive and has immune mediated and genetic basis.
Interestingly, CSK has been shown to be mediated by increased UV light exposure, with altitude significantly affecting the prevalence of this disease. Diagnosis of CSK is often based on clinical findings and breed predisposition, as well as response to treatment.
However, in dubious cases, cytopathology or histopathology may help to confirm the suspicion, and to rule out other corneal diseases (such as pigmentary keratitis, keratoconjunctivitis sicca or chronic irritation). In fact, CSK is characterised by a lymphoplasmacytic infiltrate with concurrent fibrovascular proliferation and pigmentation. Increased numbers of plasma cells are often observed on cytopathology.
CSK can generally be controlled through medical (such as topical immunosuppressant medications, steroids) or surgical means (such as superficial keratectomy), but it cannot be cured and may lead to blindness.