6 May 2019
Steven Hancox gives a step-by-step guide to this type of surgical ligature and offers some examples of how to use it in surgery.
Steven Hancox
Job Title
Numerous types of knot can be used to create a surgical ligature. They are all types of binding knot – and various forms of these have been used for centuries whenever a rope needed to be tied around another structure (Ashley, 1944).

The surgeon’s knot is the ligature used most often in veterinary surgery, the first part of which is called a double overhand throw. The suture material is passed around the pedicle once, then the stands are passed over each other twice. More holding power exists in knots that pass around the structure twice. This family includes the miller’s knot, strangle knot and constrictor knot. The former two would be good choices to tie around a miller’s sack as they are more secure than single-pass binding knots, but relatively easy to undo. The miller’s knot, modified miller’s knot and strangle knot can also be used as surgical ligatures (Hazenfield and Smeak, 2014; Hardie, 2008).
The constrictor knot is known to be the most powerful binding knot (Ashley, 1944). This knot would be a poor choice to temporarily tie off a miller’s sack as undoing it without cutting the rope is virtually impossible. This holding power is one of the reasons the constrictor knot is an ideal candidate as a surgical ligature.
A further advantage of the constrictor knot is it has a more circular profile, compared with the D-shaped profile of the surgeon’s knot (Figures 1 and 2).
The D-shaped profile of the surgeon’s knot ligature also means tension applied to the free ends creates jerky steps, as when full tension is applied, the suture material is forced to change direction sharply at either end of the double overhand throw. Secondly, the tension created in it relies on the friction created by the double overhand throw, which is inherently weak. The double overhand throw creates sufficient friction to hold two closely apposed skin edges together when closing a routine wound as part of a normal surgeon’s knot, but it does not have enough frictional force on its own to effectively close a large vascular pedicle. A lot of the tension applied is lost after releasing the pull on the suture strands. The locking throws are a very important part of the holding power of this ligature and they need to be placed promptly, without disturbing the double overhand throw.

In a comprehensive study by Taylor and Grogono (2014), the performance of the first throw of a surgeon’s knot ligature was compared with the first throw of various other ligatures. They also compared how different synthetic suture materials affected the performance of the ligatures.
Their conclusion was a constrictor knot ligature tied with polydioxanone outperformed all the other ligatures tested by a large margin. For example, its holding power (the amount of tension remaining in the loops after pulling tight) was four times higher than the first throw of a surgeon’s knot tied with the same suture.
The performance of surgeon’s knot ligatures was found to be best with polydioxanone and worst with polyglactin.
This study also suggested modified miller’s knots and strangle knots performed relatively poorly with all the suture materials tested. They tightened readily, but did not hold their tension well.
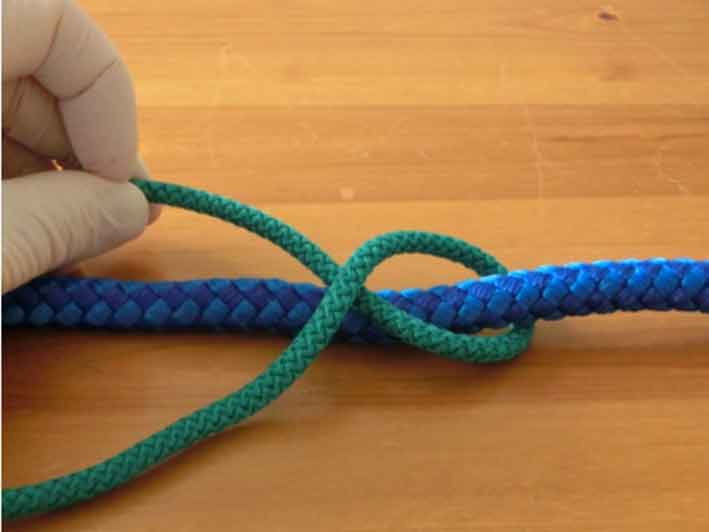
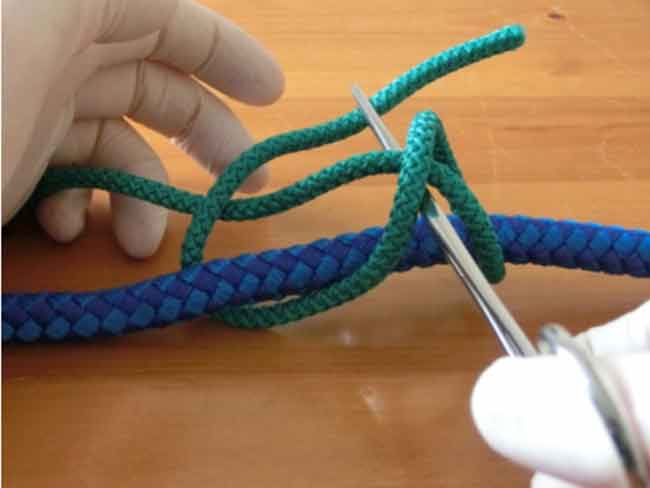
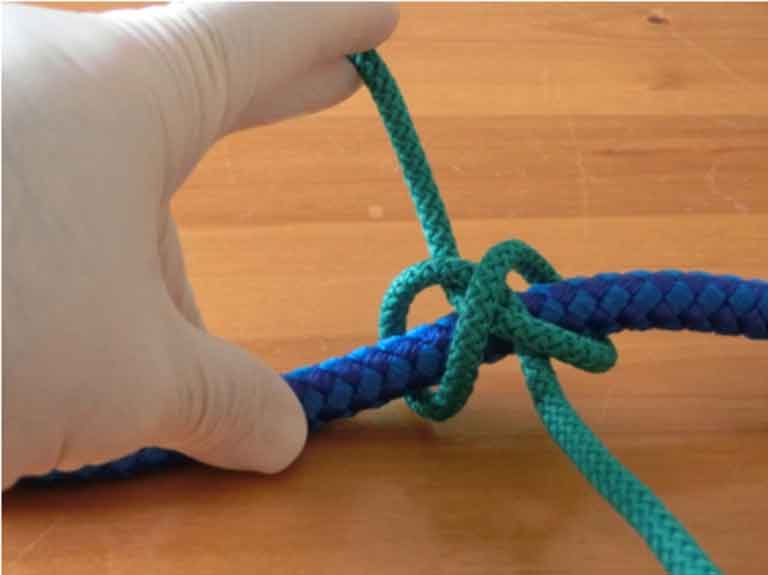
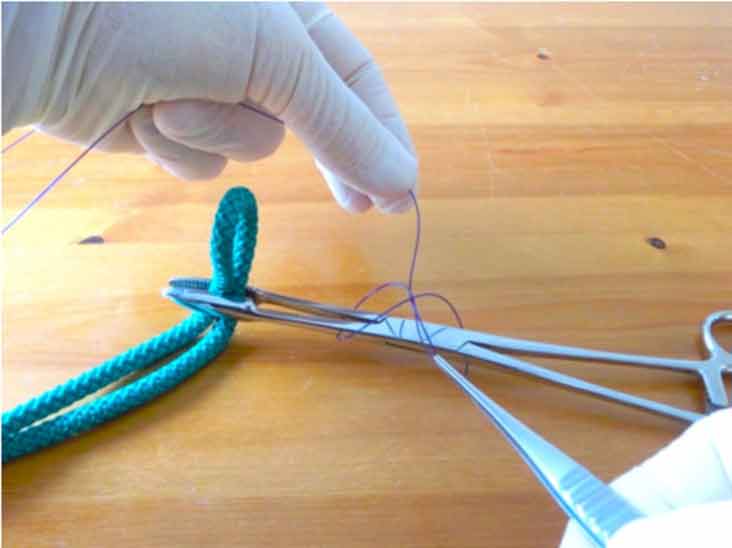
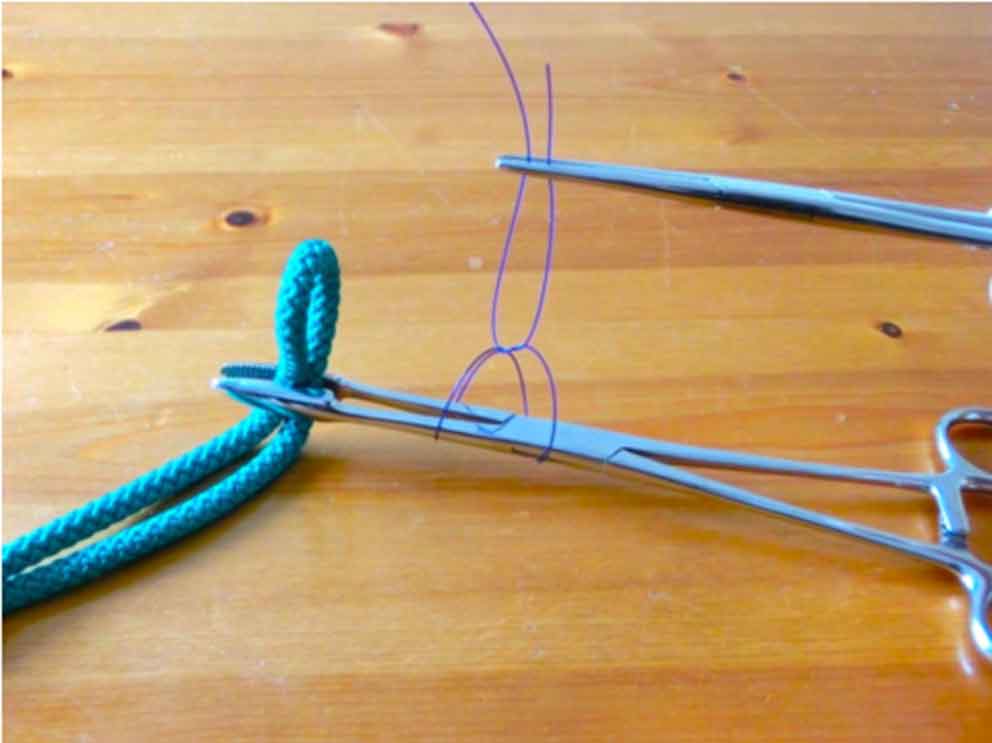
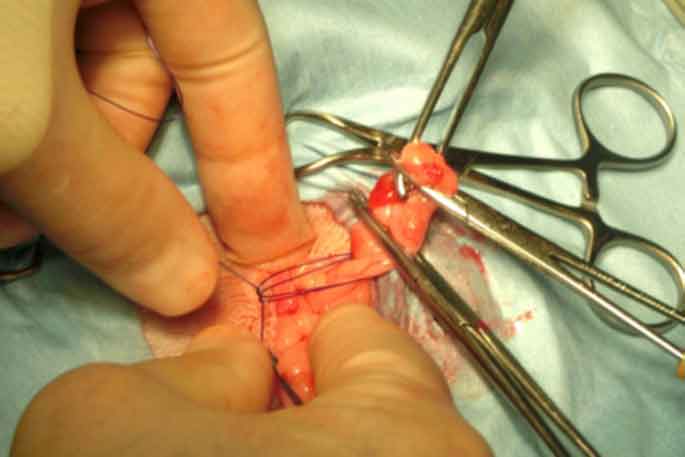
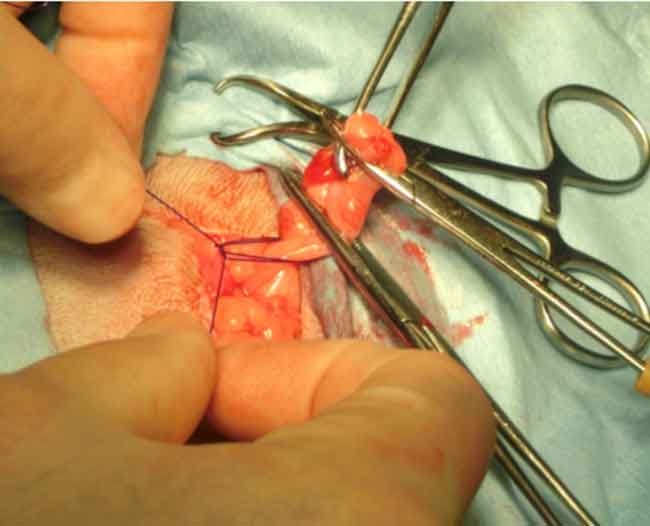
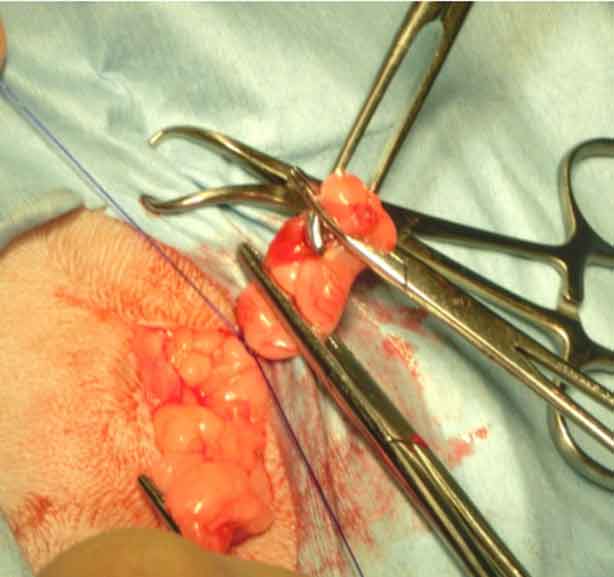
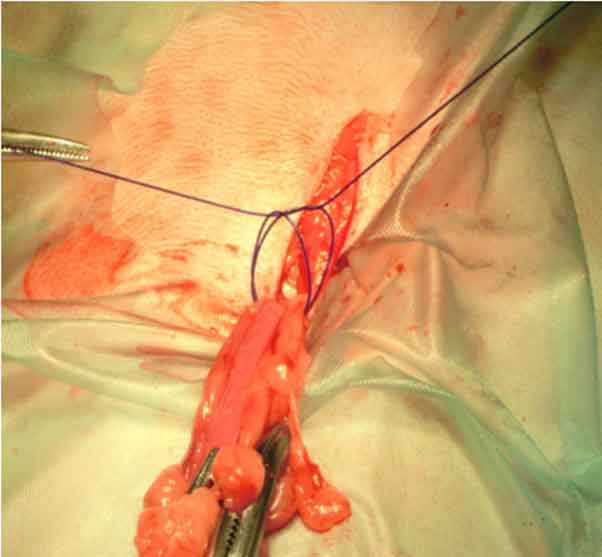
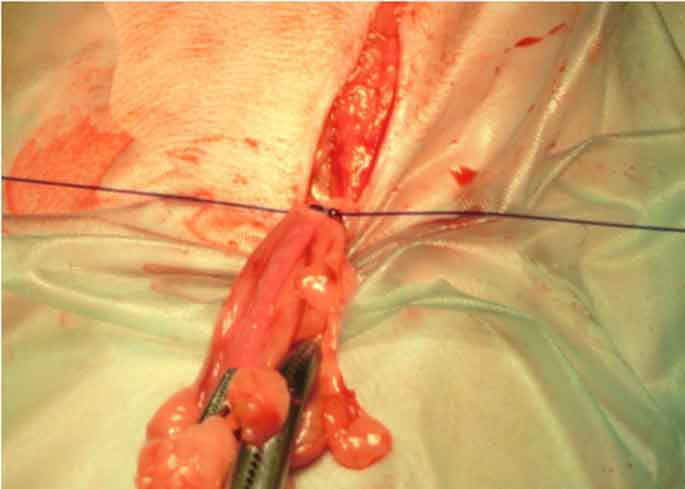
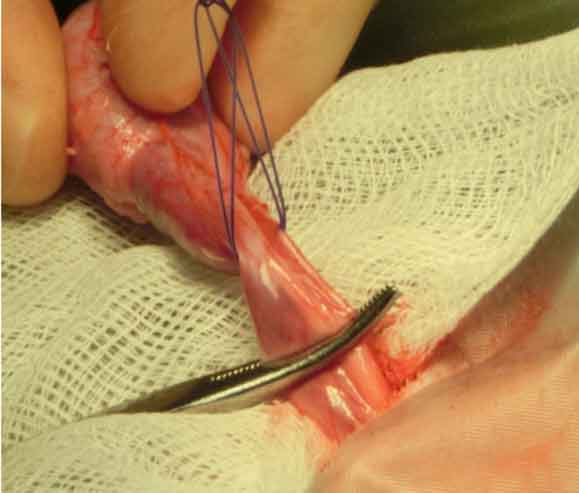
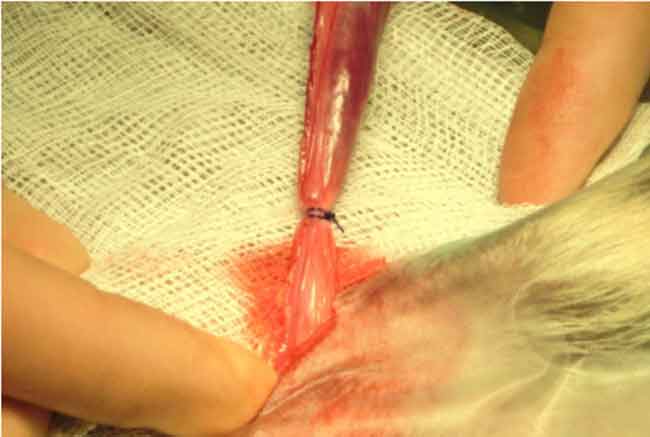
The easiest way of forming the constrictor knot ligature is to loosely pre-tie it around a pair of forceps when performing an ovariohysterectomy and around the spermatic sac/vessels when performing a castration. The free ends of the ligature are then temporarily secured using a pair of artery forceps. The ligature can then be slid into the desired position before doing the final tie (Figures 3 to 8).



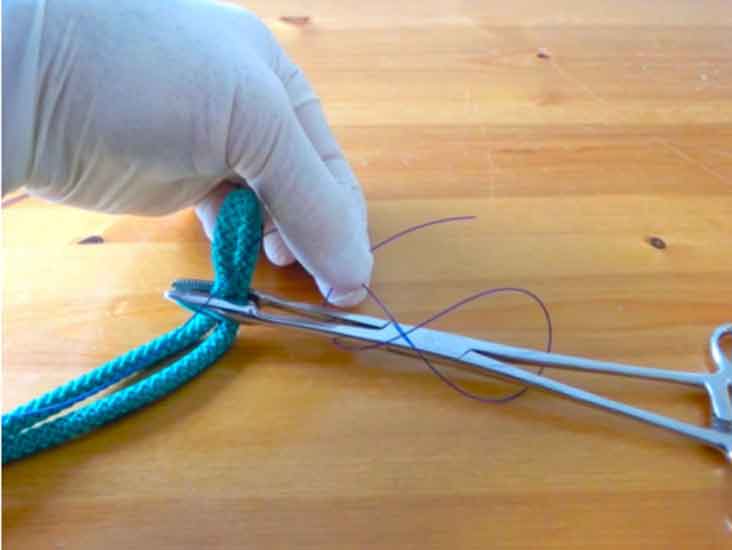
Suture tie using forceps (Figures 9 to 12); as aforementioned, polydioxanone is the synthetic suture material of choice with constrictor knot ligatures.
Using lengths of polydioxanone cut from a multi-use cassette is easier than using foil-wrapped suture packs (as well as being less expensive). When the suture is used from a cassette, cut lengths adopt a large circular shape, rather than the convoluted shape of the suture from foil packs – this makes the suture easier to handle when creating the ligature.
An important feature of the constrictor knot ligature is its holding power is maximised when the two loops are in close proximity to each other on the pedicle. One way to ensure the two loops stay close to each other is to pull up on the free ends so the pedicle is pulled gently towards the surgeon, then gradually tighten the ligature while retaining this tension. It also helps to tie it at a point where forceps have been “flashed” – that is, where the pedicle has been partially crushed by the temporary application of artery forceps.
When the constrictor knot ligature is tied with polydioxanone, the ligature is felt to tighten smoothly until an abrupt stop occurs. No need exists to strain when pulling this ligature tight – its circular shape means it reduces in diameter smoothly and the locking point is reached with relatively little effort. The smooth sensation when tightening this suture is very much different to the surgeon’s knot ligature, where a more jerky, stepped sensation occurs as full tension is achieved. The surgeon also needs to pull a lot harder to achieve full tension with a surgeon’s knot ligature and a lot of this tension is lost as soon as the surgeon stops pulling.
It is neither necessary nor desirable to pull as hard when tightening a constrictor knot ligature as compared to a traditional surgeon’s knot ligature.

The main applications of this ligature are all those where a surgeon’s knot ligature would have been used. In general veterinary practice, this will mainly be neutering procedures.

An avascular window is selected in the broad ligament caudal to the ovarian vessels (Figure 13).

The ovarian pedicle is cut just distal to the lower artery forceps after applying three locking throws, and checks are made to ensure all the ovary has been removed (Figure 21).
The constrictor knot ligature is more effective and, therefore, safer than a surgeon’s knot ligature.
Disadvantages of the constrictor knot:

he surgeon needs to learn how to tie it. When learning this knot, it is easier to tie around a horizontal structure (when using artery forceps in the aforementioned method, this allows more space in which to pre-place the ligature). It is possible to tie it around the proximal uterus without using forceps or any sectioning of the uterus, but the amount of space available is reduced.
Advantages of the constrictor knot include:
Cutting the uterus close to the ovary, so the constrictor knot ligature can be slid over the ovary, is inherently safe as this site is relatively avascular compared to the ovarian pedicle. In a routine bitch spay, if the forceps close to the ovary were loosened, little haemorrhage would occur. Furthermore, the ovarian pedicle will not disappear into the abdomen as little tension exists on it.
In a large bitch spay, the forceps are applied to the uterine horn to compress the axial/abaxial surfaces, rather than lateral/medial surfaces, as the blood vessels lie in the broad ligament on the axial aspect of the uterine horn. In a small bitch spay, it makes little difference how the forceps are applied.
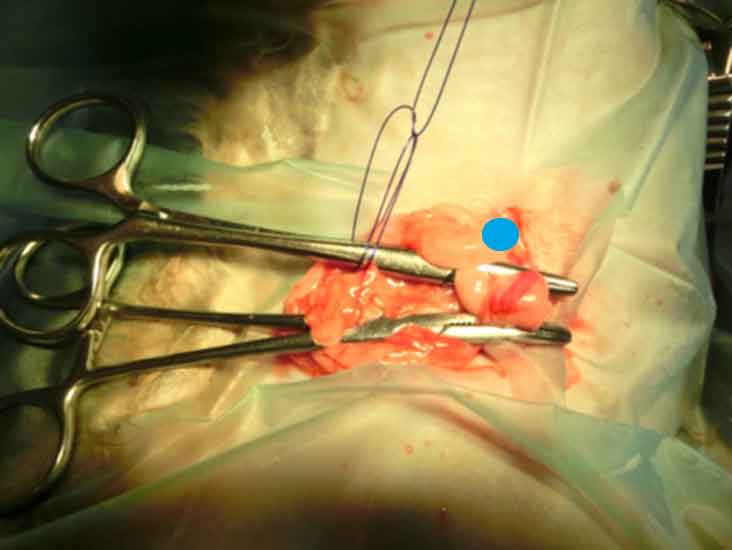
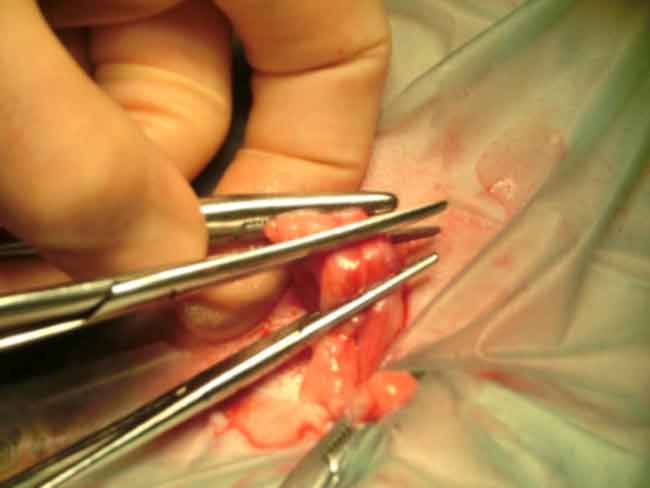
Allis tissue forceps are applied near the ovary to improve access to the ovarian pedicle. A non-scrubbed nurse can hold the Allis forceps using their little finger only. Tension applied to these forceps is checked by the surgeon. The tips of the Allis forceps are held by the surgeon while the Allis forceps are released. Two sets are required; one for each ovary.
Maximising the security of vascular ligatures is a major priority for all surgeons.
The relatively poor mechanical properties of surgeon’s knot ligatures has led to several variations to improve its security. On ovarian and uterine pedicles, it is safer to tie two surgeon’s knot ligatures, rather than one. We can also transfix ligatures so the pedicle is closed off with two smaller loops, rather than relying on one larger one.

Surgeons may still prefer to tie a second ligature in these applications – no matter what type of ligature is used. It is the author’s contention that one well-placed constrictor knot ligature is all you need for each ovarian pedicle, for the uterine body and for the testicular vessels, whether castration is performed open or closed.
A key part of the learning curve with the constrictor knot ligature is to use it for every bitch spay and dog castration. This ligature will be of most use for the larger patient where its mechanical advantages are maximised, but if the surgeon has become familiar with it on smaller dogs, the surgeon will be able to tie it confidently in any size of animal. A measurement of metric polydioxanone is suitable for most small and medium-sized dogs, with 3.5 or 4 metric being used for larger breeds.
Larger vascular pedicles can present a considerable challenge when using surgeon’s knot ligatures, as the surgeon needs to pull very hard to overcome the friction inherent in trying to close a D-shaped structure around a large circular structure. Furthermore, a lot of this tension is lost when the pull on the ligature is released. The force required to apply tension to the first throw of a surgeon’s knot ligature around a large pedicle can cause considerable concern for newly qualified vets. Hand and finger soreness can result from applying large forces to a strand of ligature material. Furthermore, any disturbance of the first throw of a traditional ligature, prior to placement of the locking throws, can result in further loosening of the ligature loop.
Because the constrictor knot ligature tightens easily (less pull means it’s much easier to tighten) and locks so well, it can greatly improve confidence in the security of pedicle ligation for inexperienced surgeons – or, indeed – any surgeon.
Research has highlighted the fact better alternatives to the surgeon’s knot ligature exist and the constrictor knot ligature outperforms all of them. It has also been demonstrated the performance of ligatures is heavily dependent on the suture material used to tie them; polydioxanone being better than polyglactin and poliglecaprone.
The main message of this article is constrictor knot ligatures are more effective than any other type of ligature.
The aforementioned technique is merely one the author has devised and been using in his practice for several years. Other techniques for tying it can be used. For example, during a bitch spay, it is possible to pre-tie it over the proximal uterus, then slide the knot over the ovary, without cutting the uterus once the surgeon is familiar with the shape of the knot.
Constrictor knot ligatures outperform ligatures based on the surgeon’s knot. They require less tension to tighten and hold the tension better after pull is released.
If they are used in procedures instead of surgical knot ligatures, they will improve the safety of that procedure – and, at the end of the day, isn’t that what we all want?