2 May 2023
Chloe Fontaine and Renata Stavinohova discuss diagnosis and treatment options for dogs in the first of this two-part series on common eye problems.

Figure 1. Bennett Cilia atraumatic forceps is used for third eyelid manipulation.
This article – divided into two parts – describes conjunctival anatomy and physiology, and discusses conjunctival diseases in dogs and cats.
The article also summarises a few practical tips for general practitioners to help them answer commonly asked questions. For example, what is the role of the conjunctiva? Why does it become inflamed? What are the causes? Are they the same in dogs and cats? And most importantly, how do you diagnose and treat conjunctivitis?
Part one describes common pathogens and their treatment in dogs. The anatomy and physiology of the conjunctiva in cats is very similar to that of dogs. However, the causes of conjunctivitis in cats are somewhat different and will be discussed in more detail in part two of this article.
“Conjunctivitis” is a descriptive term referring to inflamed conjunctiva. This condition can be caused by a variety of factors, including bacteria, viruses, fungi, allergens, parasites or tear film diseases. In many cases, multiple factors may contribute to the development of conjunctivitis.
When the conjunctiva is inflamed, it responds with classic ocular signs: discharge, blepharospasm, photophobia, chemosis and hyperaemia.

It is important to note that these signs can also be indicative of other eye conditions or diseases, which is why the complete ophthalmic examination should always be performed.
This includes measuring the tear production and using a fluorescein stain to detect any corneal abrasions or ulcers that may be contributing to the conjunctivitis.
During the ophthalmic examination, the eyelids and the third eyelid should be gently everted or lifted, and examined with appropriate magnification.
A conjunctival smear cytology, culture and sensitivity test of any discharge present may also be performed.
A conjunctival biopsy and histology is crucial to obtain appropriate diagnosis; for example, in conjunctival neoplastic lesions.
Treatment for conjunctivitis depends on the underlying cause of the condition.
The conjunctiva is characterised by a mucous membrane of loose connective tissue beneath a stratified columnar epithelium.
Depending on its location, the conjunctiva is referred to as either palpebral (lying under the eyelid), bulbar (touching the globe), or fornix conjunctiva (at the junction of the palpebral and bulbar conjunctiva; Shumway et al, 2022).
It consists of a deeper fibrous layer containing nerves and vessels, and a more superficial adenoid layer containing lymphoid follicles, which are commonly seen in cases with conjunctivitis.
Lymphoid follicles are the main component of the conjunctiva-associated lymphoid tissue (CALT). Their primary role is to act as an immune and barrier system for the ocular surface by taking up antigens via M cells and presenting them to circulating mononuclear cells. This explains why these follicles appear conspicuous during intense stimulation (Giuliano et al, 2002).

The conjunctiva also contributes to the health of the tear film and, therefore, the cornea. The goblet cells in the epithelial layer of the conjunctiva are responsible for the mucin portion of the tear film, which attaches to the corneal surface and traps debris and microorganisms.
Primary bacterial conjunctivitis is an uncommon disease in the dog (Figures 2 and 3). In most cases, bacterial conjunctivitis develops secondary to eyelid abnormalities or keratoconjunctivitis sicca (KCS). Staphylococcus species and other Gram-positive bacteria are common pathogens. Diagnosis is made by culture from a conjunctival swab or from deep tissue culture of a conjunctival biopsy. Treatment consists of topical broad-spectrum antibiotics while culture is pending (Whitley, 2000).
Fungal and viral conjunctivitis are not encountered very frequently in dogs. Other infectious causes of conjunctivitis include rickettsial diseases such as canine ehrlichiosis.
Parasitic pathogens include Thelazia callipaeda – a white, 10mm to 14mm long nematode occasionally found behind the third eyelid – in the conjunctival sac or tear duct. A monthly administration of milbemycin oxime and afoxolaner is the preventive treatment of choice (Lebon et al, 2019).

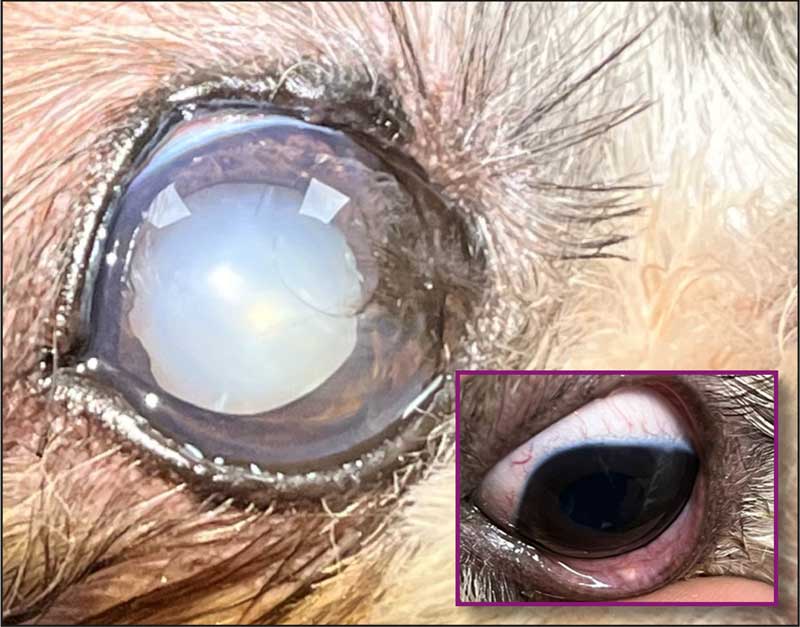
KCS or quantitative KCS dry eye is a frequent cause of conjunctivitis in the dog (Figure 4). It is a chronic condition that occurs when insufficient production of the aqueous component of the tear film exists, leading to dryness of the cornea and conjunctiva.
KCS is most commonly caused by immune-mediated destruction of the tear-producing glands – especially the lacrimal glands. However, other causes of KCS in dogs include congenital, infectious diseases such as canine distemper virus, traumatic, iatrogenic (excision of nictitating membrane gland), radiation therapy, drug induced or systemic disease (diabetes mellitus).
KCS is the most common cause of secondary bacterial conjunctivitis in dogs. However, clinical attention is often misdirected towards investigating the bacterial agent instead of conducting a Schirmer tear test and assessing the health of the cornea.
Clinical signs of KCS include blepharospasm, corneal vascularisation, fibrosis and pigmentation; and the triad of ocular signs seen in conjunctivitis: chemosis, hyperaemia and a mucoid to muco-purulent discharge (Whitley, 2000; Figures 5 and 6). This can lead to dramatic consequences, such as deep corneal ulcers and even perforation. A fluorescein test is, therefore, important to assess corneal health and integrity.
Diagnosis of KCS is made by performing a Schirmer tear test-1 (STT-1). The STT-1 is performed without local anaesthesia and measures basal and reflex tear production. If the STT value is less than 5mm per minute (mm/min), it indicates that the animal is affected by a quantitative dry eye. STT values between 5mm and 10mm strongly suggest KCS.
A diagnosis of KCS can also be made with values between 10mm and 15mm if consistent clinical signs such as corneo/limbal vascularisation, fibrosis or pigmentation are present. The treatments of choice for immune-mediated KCS are lacrimostimulants (topical ciclosporin or tacrolimus) and lacrimomimetics.
Broad-spectrum prophylactic antibiotics may be often required to control the secondary bacterial infection. Systemic analgesia may be necessary due to the painful nature of this condition.
It is essential to ensure that the owners understand that KCS requires lifelong treatment and relapses can occur (Williams, 2008). In cases that have failed to respond to medical treatment, a parotid duct transposition may be performed. In this surgery, the duct of the parotid salivary gland is repositioned from the mouth to the eye to provide lubrication.



Another cause of quantitative KCS is neurogenic dry eye caused by a lesion affecting the preganglionic parasympathetic nerve fibres, anywhere from the rostral medulla oblongata to the pterygopalatine ganglion. Dogs affected by this condition will present with unilateral ocular signs of KCS, as well as with ipsilateral xeromycteria (a dry nostril) and xerostomia (a dry mouth; Cook et al, 2004; Figures 8 and 9). The treatment includes lacrimomimetics, oral pilocarpine and lacrimostimulants (topical ciclosporin or tacrolimus). Neurotrophic dry eye due to an absent or reduced corneal sensation can also contribute to conjunctivitis.
Qualitative dry eye is less common and harder to diagnose (Figure 10). Poor tear film quality can lead to faster evaporation of the tear film and therefore drying of the cornea. It can develop secondary to meibomitis or any damage of the goblet cells or meibomian glands.
Meibomitis is a disease affecting the meibomian glands that causes a decreased lipid component in the tear film, leading to premature evaporation of the aqueous phase, although STT may still be within normal range. Meibomitis is associated with blepharitis and blepharoedema.
Qualitative dry eye also requires lifelong treatment with lacrimomimetics and temporary broad spectrum prophylactic topical antibiosis. Lacrimostimulants may also be considered.


Allergic conjunctivitis is a common clinical sign observed in dogs with atopic dermatitis or type I hypersensitivity – also known as immediate hypersensitivity – and involves immunoglobulin E-mediated release of antibodies in response to soluble antigen (Abbas et al, 2022; Figure 11). In addition to the classic conjunctivitis signs, periocular alopecia, erythema and facial pruritus is present. The primary treatment is to eliminate the allergen.

Additionally, topical lacrimomimetics and NSAIDs can be started. Topical steroids are sometimes required to control the inflammation. Systemic treatment of atopic dermatitis – such as immunotherapy, topical and oral immunomodulators – should be discussed with a dermatologist (Delgado et al, 2023).
Local drug allergic reaction can occur after topical neomycin, gentamicin, dorzolamide, timolol, thimerosal and benzalkonium (Figure 12). Clinical symptoms usually resolve when treatment is discontinued. Topical lacrimomimetics can be started to alleviate ocular discomfort.
Follicular conjunctivitis develops due to chronic antigenic stimulation in younger dogs. Prominent follicles occur on the bulbar conjunctiva of the nictitating membrane, but can present anywhere on the conjunctiva (Figure 13).
Follicular conjunctivitis is a self-resolving condition. Very rarely it can cause severe ocular discomfort and, consequently, secondary entropion. In severe cases, treatment with topical lacrimomimetics, steroids and/or NSAIDs, and systemic NSAIDs is commenced. Adjunctive analgesia (for example, paracetamol) may be also required. Ocular irritants such as chemicals, smoke, pollution, allergens or foreign particles can also contribute to follicular conjunctivitis.
Primary ocular neoplasia (melanoma, mast cell tumour, papilloma, squamous cell carcinoma, haemangioma, haemangiosarcoma or angiokeratoma) can cause irritation and contribute to conjunctivitis. Systemic neoplasia – such as multiple myeloma, lymphoma or systemic histiocytomas – will cause infiltrative conjunctival disease, which clinically presents as a conjunctivitis (Hartley and Hendrix, 2021). Conjunctival biopsy and histology is crucial to reach the diagnosis and appropriate treatment plan.

In diffuse conjunctival diseases, the biopsy is easily obtained from the lower conjunctival fornix in front of the third eyelid, which can be made to protrude by applying gentle pressure through the upper eyelid and retropulsing the globe. The protruding third eyelid will protect the cornea and this will render the sampling process easier.
Conjunctivitis can occur secondary to other ocular problems; for example, corneal and adnexal diseases, abnormal cilia, caruncular trichiasis, medial canthal pocket syndrome, lacrimal cysts, uveitis, ocular trauma, foreign bodies or nodular granulomatous episclerokeratitis (Figures 14 and 15).
Anatomic abnormalities that cause inadequate tear drainage or chronic irritation can also directly affect the conjunctiva. Petechiae or hyposphagma (subconjunctival haemorrhage) can occur secondary to conjunctival irritation; for example, local drug allergic reaction or due to coagulopathies (Figure 16).
Systemic infectious diseases – for example, leishmaniasis – have been shown to cause conjunctivitis, blepharitis, keratitis, retinitis, and anterior uveitis. Orbital diseases such as mucoceles (for example, zygomatic mucocele) or retrobulbar cellulitis or abscess, also contribute to conjunctivitis (Figures 17 and 18).
In conclusion, the conjunctiva in dogs can be involved in many disease processes. A systematic and logical approach is critical to allowing the cause of conjunctivitis to be narrowed down.
History and clinical signs should be reviewed first, then a thorough ophthalmic and physical examination should follow, including performing the critical diagnostic tests.





