10 Mar 2020
Michael Day looks at pathogens old and new associated with this condition, as well as diagnosis and vaccination.
Michael Day
Job Title
Image: Reddogs / Adobe Stock
Research over the past 10 years has revealed many more pathogens may be implicated in the aetiology of “kennel cough” than previously thought. The advent of more sophisticated diagnostic technologies, such as PCR testing, has suggested more than 20 different viruses, bacteria and mycoplasmas may contribute to this common respiratory disease.
It is clear we should now be thinking of kennel cough as a multifactorial complex and adopt “canine infectious respiratory disease complex” (CIRDC) as the preferred terminology.
Despite this enhanced insight into disease aetiology, no recommendations exist to change the clinical management of acute cases or the environmental advice for group situations, and the options for protection via vaccines remains limited. In practice, vets should use the annual health check as an opportunity to ask owners whether their pets are likely to be mingling with other dogs at, for example, shows, social events or grooming parlours in the coming year, and offer suitable non-core vaccines to those at risk of CIRDC. Recommending appropriate vaccination will benefit the individual dog and deliver the benefit of herd immunity to the population as a whole.
Our understanding of “kennel cough” has advanced significantly over the past decade.
The application of new diagnostic technologies, such as PCR testing, has facilitated insight into the pathogenesis of this common canine condition, and into the respiratory microbiomes of healthy dogs.
During this time, a gradual shift in canine lifestyles has also occurred, with more dogs taking part in group activities, such as puppy parties, attending grooming parlours or dog parks, “doggy day-care” and commercial dog walking, all of which increase the risk of transmission of respiratory infection.
As a result, the historical term “kennel cough” is being replaced with the more accurate descriptor “canine infectious respiratory disease complex” (CIRDC). CIRDC emphasises the complex nature of this disease – which involves host, pathogen and environmental factors – the latter including the lifestyle and infectious disease exposure risk of the individual, socially active dog.
The basic clinical presentation and therapeutic management of CIRDC has remained largely unchanged, but the potential involvement of a wider range of pathogens, and evidence of emerging pathogens, poses a number of challenges for vets with regard to diagnosis, prevention and advice for owners.
The latter challenges are complicated by an increasing owner aversion to vaccination, which some colleagues will have experienced and may represent a “halo effect” triggered by concerns over vaccine safety in children. These concerns may be addressed in part by new developments in vaccinology, such as the recent launch of an oral vaccine, which offers an alternative approach to vaccine delivery.
Intensive research by groups in the US, EU and UK over the past 10 years has shown the variety of pathogens that may potentially be involved in CIRDC is changing as new agents emerge and the importance of traditional pathogens shifts.
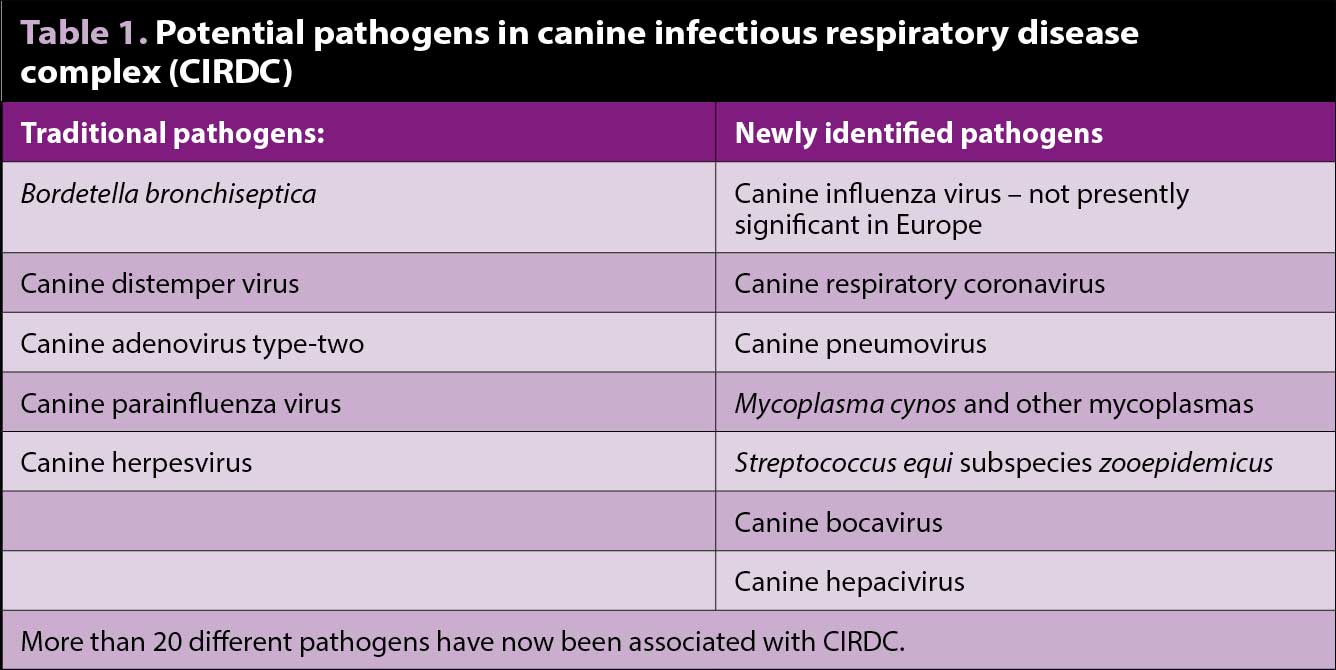
To date, more than 20 different agents that may be involved in CIRDC have been identified, including viruses, bacteria and mycoplasmas (Table 1).
Although Bordetella bronchiseptica, canine adenovirus type-two (CAV-2), canine distemper virus (CDV), canine herpesvirus (CHV) and canine parainfluenza virus (CPiV) are still considered to be important agents involved in the disease, others have now been implicated.
These new pathogens include canine influenza virus (CIV), canine respiratory coronavirus (CRCoV), canine pneumovirus (CnPnV), Mycoplasma cynos and other mycoplasmas, and Streptococcus equi subspecies zooepidemicus. Canine bocavirus and canine hepacivirus have also been isolated and associated with respiratory disease in dogs (Priestnall et al, 2014). Co-infections, with two or more pathogens in any one case, is a well-recognised occurrence (Maboni et al, 2019).
CIV infection is a major problem in Asia and the US, where outbreaks of infection caused by influenza A viruses H3N8 and H3N2 have occurred. H3N8 infection was thought to have spread to dogs from horses and an historical outbreak occurred in foxhounds in the UK in 2002 (Daly et al, 2008). CIV is not a significant pathogen in Europe (Mitchell et al, 2017), but surveillance must be maintained for any potential emergence.
CnPnV and CRCoV spread particularly well in multi-dog establishments, and are now thought to be important aetiological agents of CIRDC. M cynos is commonly found together with other CIRDC pathogens in dogs in Europe – especially in younger and kennelled dogs – and has been suggested to be a significant canine respiratory pathogen. S zooepidemicus appears to be a particular issue where dogs are kept close to horses and may cause severe pneumonia.
Although some of the agents, such as CIV and other viruses, could be described as “emerging”, no evidence exists to suggest the basic clinical presentation of CIRDC is changing significantly or that the current approach to case management requires any major adjustment.
CIRDC is most often a mild, self-limiting disease with characteristic clinical presentation, although more severe forms of canine respiratory infection do sometimes occur.
As with respiratory disease complexes in other animals, it is thought that primary pathogens infect the upper respiratory tract and compromise mucociliary clearance, and, therefore, predispose to colonisation by secondary agents, leading to potential infection of the lower airways, with consequent risk of pneumonia or chronic respiratory disease. However, the fact that more pathogens are involved than previously thought does present a number of challenges with regard to diagnosis and prevention.
The techniques used by research groups to uncover the involvement of new pathogens in CIRDC should, theoretically, provide a means of identifying those causative agents in outbreak situations and enable disease surveillance by assessing the prevalence of specific agents. However, in practice, the situation is not so straightforward.
Testing of nasal, oropharyngeal or conjunctival swabs for viral and bacterial pathogens by PCR, and submission of samples for bacterial culture has shown many of these agents are also present in the respiratory tract of healthy dogs (Lappin et al, 2017).
Testing for the presence of serum antibody against the pathogens provides information about previous exposure (as opposed to confirming active infection) and has a role in performing seroprevalence surveys for CIRDC. In fact, the majority of these pathogens appear to form part of the normal respiratory microbiome of healthy dogs and have often been detected in control groups in prevalence studies using PCR (Mitchell et al, 2017).
Although we have access to PCR (often as a screening “respiratory panel”) and serology, in addition to traditional bacterial culture or virus isolation techniques, the challenge is in how to interpret the results of such tests and how to apply that interpretation in practice. For individual cases, this level of testing is relatively expensive and unlikely to alter the standard symptomatic management of acute cases. Where decisions need to be taken for a larger population, for example, outbreaks in kennels, then the resulting insight could perhaps help to devise a more targeted preventive strategy.



Prevention of CIRDC might involve minimising risk factors in the lifestyle of the individual dog, together with vaccination.
CIRDC is not a vaccine-preventable disease because, at present, we can only vaccinate against a small number of the potential pathogens (that is, CDV, CAV-2, CPiV, B bronchiseptica and CHV). CDV and CAV-2 are part of the group of core vaccines for dogs (also including canine parvovirus type-two), and will be routinely administered to all puppies and adult dogs in accordance with current guideline recommendations (Day et al, 2016).
The core vaccines produce robust and long-lived sterilising immunity (that is, prevent infection). CHV vaccination is considered only in the context of breeding kennels to reduce deaths of neonatal puppies associated with this viral infection. Therefore, the only decisions that vets really need to make about respiratory vaccines are whether to apply non-core vaccines (that is, CPiV and B bronchiseptica) to dogs with an at-risk lifestyle (as aforementioned).
Although these non-core vaccines are less potent than core vaccines, they can reduce the severity of the illness and shedding of pathogens, and so are a key component for the management of at-risk animals. Unlike core vaccines, which have a licensed minimum duration of immunity of three years, all non-core vaccines must be administered on an annual basis to adult dogs. Respiratory vaccines are designed to induce protective mucosal IgA (and IgG) immune responses, a systemic IgG response and immunological memory to the vaccine antigen.
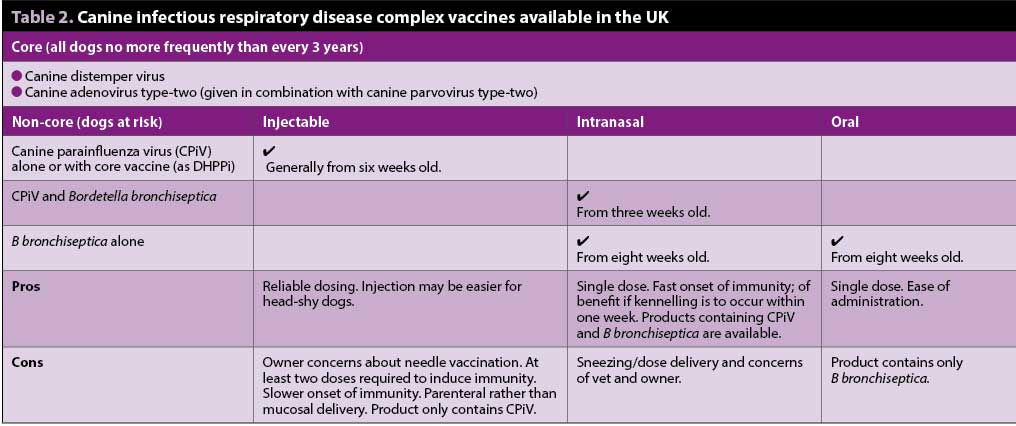
In the UK, CPiV vaccine is available as a modified live virus (MLV) injectable single antigen product or is formulated in combination with injectable core vaccines (for example, as DHPPi vaccine). B bronchiseptica is available as a live attenuated intranasal preparation either alone, or in combination with MLV CPiV. Recently, we have seen the launch of an orally administered live attenuated B bronchiseptica vaccine, giving an alternative delivery route for this vaccine component (Table 2).
Although intranasal and oral vaccines have different routes of administration, both are distributed to the pharyngeal mucosa and regional lymphoid tissue, and would be expected to induce protective respiratory mucosal immunity. Published comparative challenge studies support the efficacy of oral B bronchiseptica vaccination (Larson et al, 2013; Scott-Garrard et al, 2018).
Recent years have seen an increase in owner concerns over the safety of companion animal vaccines, partly fuelled by similar debates in the media over the potential side-effects of childhood vaccination. The resulting “vaccine hesitancy” has led to reduced herd (population) immunity and outbreaks of human measles virus infection in many countries. Concerns about companion animal herd immunity have been highlighted by the PDSA Animal Wellbeing (PAW) Report, which revealed a year-on-year decline in vaccine uptake in dogs (PDSA, 2019).
In 2019, 72% of dogs were given a primary course of vaccination, compared with 88% in 2016. Of those that did receive a primary course, 19% did not have subsequent regular boosters. Reasons for not having vaccination included concerns about vaccine side effects (13%), a feeling that the risks outweighed the benefits (13%) and simply not agreeing with the concept of vaccination (13%). These are all objections that can be addressed face-to-face with owners at the annual health check consultation.
Intranasal vaccine delivery can avoid owner concerns associated with pain or safety associated with needle injection, but it may induce sneezing in some dogs, which can make the vet feel uncomfortable and raise questions as to whether a sufficient amount of antigen was successfully delivered.
On the other hand, some intranasal products contain both B bronchiseptica and CPiV antigens, and delivery via the intranasal route may start to induce immunity within a few days and certainly much sooner than parenteral vaccination.
It is possible this early onset may be a result of stimulation of local innate immune pathways, rather than activation of adaptive immunity, which will take a little longer. This early onset of immunity could be beneficial if the dog is due to go into a boarding kennel within the following week. Some of the intranasal products may be given to puppies as a single dose from as early as three weeks of age.
The new oral vaccine is monovalent (that is, contains just B bronchiseptica) and may be given to puppies from eight weeks of age. It has an onset of immunity of around three weeks, but is very easy to give, is not distressing for the dog and removes the issue with sneezing.
This new route of administration provides a way of protecting animals effectively, and, at the same time, is a more positive experience for the dog, owner and the vet. This, in turn, could help improve compliance, and, therefore, the levels of protection within the general population.
An added advantage of increasing herd immunity for CIRDC is the potential for reduction in antimicrobial usage in those affected dogs in which antibiosis is deemed necessary. Vaccination may, therefore, have an indirect role in reducing the likelihood of development of antimicrobial resistance.
Vets and owners will now have to decide which combination of non-core respiratory vaccines is most appropriate for the individual at-risk puppy or adult dog. Continued surveillance is required throughout Europe to track the evolution of pathogens involved in CIRDC and to ensure we are developing tools that will optimise our ability to protect against this common disease complex.
It is clear we should now adopt “canine infectious respiratory disease complex” as the preferred terminology for this widespread and common disease of the dog.
The annual health check consultation is an ideal opportunity to ask owners whether their pets are likely to be mingling with other dogs at, for example, shows, social events or grooming parlours in the coming year. With that risk assessment in mind, it is then possible to discuss how best to protect their pets against this disease, including the most appropriate vaccination programme.
Recommending appropriate vaccination will benefit the individual dog and deliver the benefit of herd immunity to the population as a whole.