Companion animal patient eye conditions part 2: cats
Mike Rhodes BVM&S, CertVOphthal, DipECVO, MRCVS provides an overview of the most common feline disorders, including clinical signs, causes and treatment.
Mike Rhodes
Job Title
Figure 1. Lower feline entropion, left eye.
This article – the second in a two-part series – discusses some of the more common ophthalmic conditions seen in cats.
For ophthalmology conditions in dogs, see part one of this article (VT50.09) and for rabbits, refer to the article “Guide to ophthalmology in rabbits” (Maini and Hartley, 2019).
Clinical tip
As a general rule, most ocular disease in cats is associated with feline herpesvirus (FHV-1). PCR testing for FHV-1 can prove problematic due the possibility of false positives and false negatives. Therefore, some ophthalmologists advocate not testing for FHV-1, but instead treating for the virus if the clinical signs are consistent with FHV-1 infection.
Entropion
Entropion (Figure 1) is inversion of the eyelid(s), resulting in ocular irritation and corneal disease due to direct contact of the eyelid hairs. Entropion is much less common in cats compared to dogs.
Clinical tip
When performing surgical correction of entropion in cats (see further on) always take away more eyelid tissue when compared to a similar procedure in a dog.
Clinical signs
Clinical signs include:
blepharospasm (relieved by the application of topical local anaesthetic solution – for example, proxymetacaine hydrochloride 0.5 per cent
corneal ulceration and keratitis (the position of which corresponds to where the eyelid hairs contact the ocular surface)
corneal sequestrum formation (see further on)
increased tear production, epiphora and periocular wetting
increased blink rate
self-trauma
Causes
Three main clinical presentations exist in cats with entropion:
Older cats that lose orbital tissue (most common) – the resultant enophthalmos causes the lower eyelids to turn inwards (secondary entropion).
Cats that suffer from chronic painful ocular disease – for example, ulcerative keratitis associated with FHV-1.
Breed-related – some cat breeds, such as the Maine Coon, have excessive facial “jowl” tissue that can result in lower entropion. Persians have also been reported to have a breed-related predisposition to lower entropion.
Treatment
Figure 2. Conjunctivitis, right eye.
Treatment options include the following.
Permanent surgical correction
While the underlying cause of the entropion needs to be addressed, surgery is always required to resolve the entropion. In the author’s experience, an exaggerated Hotz-Celsus procedure will suffice to correct lower entropion in cats, but sometimes combination surgery with eyelid shortening (wedge excision) is also required. As previously mentioned, more eyelid tissue needs to be excised when comparing similar procedures in dogs.
A Hotz-Celsus combined with a lateral canthal closure has been reported as another very effective means of correcting feline entropion (White et al, 2012).
Surgical management of concurrent corneal sequestrum
Chronic feline entropion cases often develop associated corneal sequestra (see further on).
A superficial keratectomy can be performed at the same time as the eyelid surgery, but appropriate microsurgical training and specialist equipment are required for such procedures. If the corneal sequestrum is very deep (more than 75 per cent corneal depth), the author favours a conjunctival pedicle grafting procedure at the same time.
Conjunctivitis
Conjunctivitis (Figure 2) is relatively common in cats, and is usually primary and infectious (compared to secondary or other ocular or systemic disease processes in the dog).
Clinical tip
The two most common infectious causes of feline conjunctivitis include FHV-1 and Chlamydophila felis; the latter can never cause corneal disease, whereas FHV-1 can cause conjunctival and/or corneal disease.
Infectious/primary (most common) – FHV-1 and C felis are the most common causes of primary infectious conjunctivitis in cats. Other pathogens have also been implicated, including feline calicivirus, Mycoplasma species, Staphylococcus epidermidis, B-haemolytic Streptococcus species and non-haemolytic Streptococcus species, but in the author’s opinion, these are most likely opportunistic commensals rather than primary pathogens.
Entropion.
Eyelid agenesis.
Tear film deficiency (qualitative).
Eosinophilic conjunctivitis (see further on).
Symblepharon – loss of the corneal limbal stem cells following neonatal and/or severe FHV-1 infection leads to conjunctival adhesions between the eyelids, conjunctiva and cornea.
Lipogranulomatous conjunctivitis – multifocal nodules develop within the upper palpebral conjunctiva adjacent to the eyelid margins in both eyes.
Neoplasia – although rare in cats, primary conjunctival neoplasia includes squamous cell carcinoma, melanoma and peripheral nerve sheath tumours. Secondary tumours have also been reported including conjunctival lymphoma (B-cell).
Trauma – for example, a cat fight, air gun pellet or road traffic collision.
Treatment
Address and treat the underlying cause
FHV-1 conjunctivitis can respond favourably to a “less-is-more” approach. If the clinical signs are not severe, stopping all treatment can reduce stress levels, allowing the cat to fight an effective immune response to the virus.
If this approach fails, the author opts for either topical 0.15 per cent ganciclovir eye gel 5g three to four times daily for 7 to 14 days, or oral famciclovir 90mg/kg twice daily for five days. Please note in-vivo studies demonstrating the effectiveness of ganciclovir versus FHV-1 are lacking, but anecdotally it can work well in some cases and is relatively inexpensive.
C felis-associated conjunctivitis is best treated with oral doxycycline. Topical treatment is not recommended because this infection is a systemic disease. Bova UK offers a chicken-flavoured oral paste that may reduce the risk of oesophageal irritation seen with this drug.
In cases of entropion and eyelid agenesis, surgical intervention is warranted.
If due to an underlying tear film deficiency, topical lacrimomimetic therapy should be considered.
Eosinophilic conjunctivitis can be treated with topical corticosteroids or ciclosporin. Megestrol acetate can be a very effective alternative, but is not recommended as a first-line treatment due to the reported side effects.
Once symblepharon has formed, surgical intervention is very rarely successful due to the rapid reformation of these adhesions.
Figure 3. Dendritic corneal ulceration, right eye.
Lipogranulomatous conjunctivitis is best treated via surgical curettage of the nodules.
Conjunctival neoplasia is rarely cured with local surgical excision. Local recurrence is common and metastasis can occur – for example, feline conjunctival melanoma.
Corneal ulceration – indolent superficial ulcers
Clinical tip
Feline superficial ulcers are not the same as canine spontaneous corneal chronic epithelial defects – DO NOT perform a keratotomy or corneal burr in a cat because you are likely to induce a corneal sequestrum that will further delay the epithelial healing process.
Clinical signs
Clinical signs include:
dendritic corneal ulcer (Figure 3; these linear, branching, fluorescein-positive lesions are pathognomonic for FHV-1 infection)
superficial corneal ulcer (Figure 4) with loose, non-adherent epithelial edges
blepharospasm (these ulcers can be more painful than deeper lesions due to the more superficial distribution of the sensory nerves within the corneal surface)
conjunctival hyperaemia
ocular discharge (serous, mucoid, mucopurulent)
corneal neovascularisation
corneal sequestrum formation
Causes
Figure 4. Superficial corneal ulcer, right eye.
Causes include:
FHV-1– the virus replicates within the corneal epithelium resulting in dendritic corneal ulceration in the very early part of the disease process. These ulcers quickly develop into larger, superficial geographic ulcers that are very painful, often becoming chronic.
Breed related – brachycephalic breeds of cat – for example, Persians – have been shown to have significantly reduced corneal sensation when compared with domestic shorthair cats. Over a prolonged period of time this leads to chronic central corneal exposure and poor corneal surface health. Indolent superficial corneal ulceration then ensues in combination with corneal sequestrum formation.
Entropion (previously mentioned).
Upper eyelid agenesis.
Treatment
Surgery will be required in cases of entropion or upper eyelid agenesis.
FHV-1-related indolent corneal ulcers can be managed with topical ganciclovir 0.15 per cent eye gel three to four times daily for 7 to 14 days, or oral famciclovir 90mg/kg twice daily for five days.
A broad-spectrum topical antibiotic agent is also recommended – for example, chloramphenicol ointment twice daily. The loose epithelial edges of the lesion should be debrided following the placement of topical local anaesthetic solution every two weeks to help reduce the viral load.
The placement of a bandage contact lens can also be beneficial. Given these cats are very painful, a concurrent oral NSAID (if appropriate for the case) is recommended.
As previously mentioned, a tendency exists to “overtreat” these cases, resulting in significant stress to the individual cat. A “less-is-more” approach could be considered if the aforementioned treatment regime fails to resolve the clinical signs.
Figure 5. Eosinophilic keratoconjunctivitis, left eye.
The author prefers a surgical approach with superficial corneal ulcers in brachycephalic cats refractory to medical treatment in the form of a superficial keratectomy in combination with a conjunctival grafting procedure.
Appropriate microsurgical training and specialist equipment is required for such surgery – therefore referral is advised.
Eosinophilic keratoconjunctivitis
Eosinophilic keratoconjunctivitis (EK; Figure 5) is a proliferative keratoconjunctivitis unique to cats and is marked by eosinophilic inflammation.
Clinical tip
The white “cottage cheese-like” corneal lesions often take up fluorescein stain and are falsely diagnosed as corneal ulcers. Typically, cats with EK are non-painful, whereas cats suffering from ulcerative keratitis exhibit blepharospasm.
Clinical signs
Clinical signs are:
often unilateral, but can be bilateral
proliferative white/pink, raised lesions arising from the dorsolateral limbus
multifocal white (“cottage cheese-like”) corneal lesions that retain fluorescein
the affected eyes are often open and comfortable
the third eyelid and upper/lower eyelids can also become involved.
Causes
This presumably immune-mediated condition results in eosinophilic inflammation involving the conjunctiva, cornea, eyelids and third eyelid. Some authors postulate a link with FHV-1, but this is very difficult to prove given the ubiquitous nature of FHV-1.
Treatment
Topical corticosteroids or ciclosporin work well. Megestrol acetate can be a very effective alternative, but is not recommended as a first-line treatment due to the reported side effects.
Corneal sequestrum
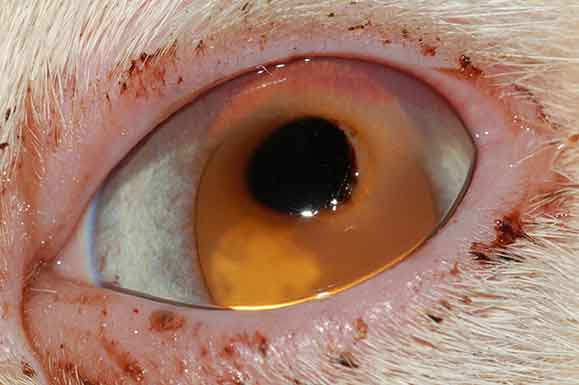
Figure 6. Dense central corneal sequestrum.
Corneal sequestrum (Figure 6) is a condition that presents as an area of corneal discolouration (amber, brown-to-black) and is associated with corneal necrosis.
The exact nature of the pigment remains unknown.
Clinical tip
If surgery is not an option to remove a corneal sequestrum then medical management with a topical broad-spectrum antibiotic ointment twice daily – for example, chloramphenicol – is acceptable in the hope that an associated corneal neovascular response leads to sloughing of the sequestrum from the corneal surface. However, owners need to be warned that in some cases the sequestrum can progress to involve the full corneal thickness, resulting in a focal point of weakness and a spontaneous corneal perforation.
Clinical signs
Clinical signs include:
area or brown corneal discolouration (diffuse and/or focal involving varying depths of the cornea)
blepharospasm (especially if associated with corneal ulceration)
superficial corneal ulceration
progressive corneal ulceration
spontaneous corneal perforation (less common)
conjunctival hyperaemia
ocular discharge (serous, mucoid, mucopurulent)
corneal neovascularisation
Causes
Causes are:
FHV-1 infection
breed related (brachycephalic breeds, such as Persians)
Always try to identify and treat the underlying cause if possible – for example, surgical correction of lower eyelid entropion (previously mentioned).
Otherwise, two treatment options exist to manage corneal sequestra in cats:
Conservative medical therapy in the hope the corneal sequestrum is reached by a corneal neovascular response and sloughs away from the corneal surface of its own accord. A topical broad-spectrum antibiotic ointment twice daily – for example, chloramphenicol – would suffice +/− the placement of a bandage contact lens and systemic analgesia if concurrent corneal ulceration is present.
Surgical intervention – the author favours a localised keratectomy to remove the majority of the discoloured corneal tissue, followed by the placement of a small conjunctival pedicle graft into the centre of the site. In cats specifically, this type of conjunctival graft is very likely to become almost transparent in time and can be left in-situ. Appropriate microsurgical training and specialist equipment is required for such surgery – therefore referral is advised.
Uveitis
Uveitis refers to inflammation of the uveal tissue, and occurs when the immune privilege mechanisms for the eye become overwhelmed and the blood-ocular barrier breaks down.
Figure 8. Anterior lens luxation.
The principles of uveitis are similar in cats as they are for dogs, but the clinical signs are much less noticeable.
Clinical tip
Due to the insidious nature of feline uveitis, affected individuals often present very late on in the disease process manifesting as apparently very different ocular conditions – for example, a corneal ulcer due to chronic secondary glaucoma and globe enlargement – the underlying cause actually being chronic anterior uveitis (Figure 7) or an anterior lens luxation (Figure 8) – again due to underlying chronic anterior uveitis.
Clinical signs
Clinical signs include:
keratic precipitates (often obscured by the third eyelid)
anterior chamber fibrin
aqueous flare
hyphaema
hypopyon
rubeosis iridis (iris neovascularisation)
iris nodules
iris hyperpigmentation
inflammation of the anterior vitreous (pars planitis – “snow-banking”)
miosis
reduced intraocular pressure
cataracts
chorioretinitis
retinal detachment
Causes
Although idiopathic (lymphoplasmacytic) uveitis is relatively common in cats, infectious and neoplastic causes are more likely when compared to the dog.
A topical NSAID – for example, bromfenac. This type of drug, although not quite as potent as a corticosteroid, is preferred in cats by the author due to the risk of FHV-1 recrudescence with corticosteroids.
Topical corticosteroid – for example, prednisolone acetate. This should only be used if the cornea is fluorescein negative and for short periods in cats due to the risks of FHV-1 recrudescence.
Systemic NSAIDs – these drugs are the first choice in a cat with uveitis until an underlying infectious cause has been ruled out. However, care should be taken in cases of gastrointestinal and/or renal disease. In addition, these drugs can affect platelet function.
Systemic corticosteroids – ideally systemic corticosteroids should only be used once an underlying infectious cause to the uveitis has been ruled out, and only if the systemic NSAIDs and topical treatment fail to control the clinical signs.
Systemic immunomodulatory drugs – the author has had some good success with oral ciclosporin as a long-term treatment option in cases of immune-mediated anterior uveitis in cats.
Glaucoma
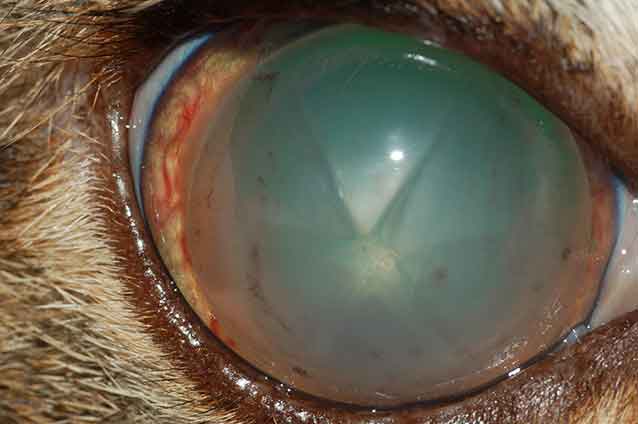
Figure 9. Chronic glaucoma, left eye.
Glaucoma is much less common in cats than dogs and is usually secondary. The points already discussed in dogs are also applicable in cats, but, like uveitis, the clinical signs are much less obvious.
Clinical tip
A slightly dilated pupil and associated anisocoria (altered pupil sizes between the two eyes) is the most common indication of early glaucoma in cats.
Clinical signs – acute
Acute clinical signs include:
mydriasis
anisocoria (unilateral cases)
reduced direct pupillary light reflex (caused by iris sphincter muscle paralysis due to a high intraocular pressure)
Ideally, one should try to address the underlying cause, but cases of feline glaucoma often present at very advanced stages of the disease process. This, coupled with the fact very few effective medical options in cats exist, often results in enucleation.
Clinical tip
The retrobulbar optic nerve is very short in the cat, so care should be taken during eye removal surgery to avoid placing traction on the optic nerve, which could result in blindness to the other eye (via optic chiasmal damage). This is especially so in chronic glaucomatous (Figure 9) cat eyes. The author often decompresses the globe prior to surgery by carefully removing aqueous humour via a small gauge needle and syringe.
Treatment includes:
medical treatment – topical treatment is restricted to dorzolamide and dorzolamide/timolol combination, but can result in bradycardia due to systemic absorption of the timolol
surgical intervention:
enucleation
laser cyclophotocoagulation (endoscopic or transscleral). Recent advances using a micropulse transscleral laser much earlier in the disease process is showing some promise
Hypertensive ocular disease
Figure 10. Hypertensive retinopathy.
The eye is a major target organ for systemic hypertension, so hypertensive ocular disease is not uncommon in cats.
Clinical tip
Cats with chronic hypertensive retinopathy (Figure 10) develop total retinal detachment and associated blindness in the affected eye(s). However, typically one eye detaches a long time before the other, during which time the cat appears visual.
The owner will only notice the cat has gone blind when the second retina detaches. This is important when giving advice to the owner regarding return of vision once the systemic hypertension is hopefully controlled and the retinas re-attach. If the first retina has been detached for many months then it is less likely to regain vision as compared to the most recent retinal detachment that should regain vision if treated promptly.
Clinical signs – early
Early clinical signs include:
retinal “target lesions”
flat, bullous retinal detachments
retinal haemorrhage (pre, intra and sub)
vitreal haemorrhage
iris haemorrhage
mydriasis
reduced direct pupillary light reflex
reduced vision
Clinical signs – chronic
Chronic clinical signs include:
total retinal detachment
hyphaema
secondary glaucoma
Causes
Causes include systemic hypertension secondary to:
renal disease
hyperthyroidism
idiopathic (no underlying cause identified, but possible early renal)
Treatment
Address the underlying cause and treat with antihypertensive therapy, aiming for a systolic blood pressure of less than 160mmHg.
Oral amlodipine – at an initial dose of 0.125mg/kg every 24 hours (increasing up to 0.25mg/kg every 24 hours).
Oral benazepril – if the amlodipine fails to control the blood pressure then benazepril can be added, especially if concurrent proteinuria is present.
Acknowledgements
The author would like to thank colleagues Heidi Featherstone, Christine Heinrich and Peter Renwick for some of the photographs used in this article.
Due to the low number of topical medications licensed for ocular use in animals, the reader is directed to prescribe appropriate treatment via the prescribing cascade.