Companion animal patient eye conditions part 1: dogs
Mike Rhodes BVM&S, CertVOphthal, DipECVO, MRCVS in the first of a two-part article, provides an overview of the most common canine ocular disorders, including clinical signs, causes and treatment.
Mike Rhodes
Job Title
Figure 1. Left eye lower entropion in a 12-month-old Rhodesian ridgeback.
This article – the first in a two-part series – discusses some of the more common ophthalmic conditions seen in dogs, while part two will focus on the same in cats.
For ophthalmology conditions in rabbits, please refer to the article “Guide to ophthalmology in rabbits” (Maini and Hartley, 2019). Due to the low number of topical medications licensed for ocular use in animals, the reader is directed to prescribe appropriate treatment via the prescribing cascade.
Entropion
Entropion (Figure 1) is inversion of the eyelid(s), resulting in contact of eyelid hairs with the ocular surface leading to irritation and corneal disease.
Clinical signs
Clinical signs include:
blepharospasm (relieved by the application of topical local anaesthetic solution – for example, proxymetacaine hydrochloride 0.5%
corneal ulceration and keratitis (the position of which corresponds to where the eyelid hairs contact the ocular surface)
increased tear production, epiphora and periocular wetting
increased blink rate
self-trauma
Causes
Causes of entropion include:
Breed-related/anatomical (most common) – typically bilateral, but can be unilateral and the affected eyelids are usually overlong. It is most commonly seen in younger dogs (4 to 12 months of age) – breeds such as the Shar Pei and chow chow – but can also affect middle-aged dogs – breeds such as the Rottweiler. Due to the likely hereditary nature of breed-related entropion, dogs that undergo surgical intervention ideally should not be bred from.
Senile entropion/excessive facial droop – most commonly encountered in the English cocker spaniel, but other breeds can be affected. The facial and periocular skin loses elasticity with age, resulting in facial droop, upper eyelid entropion and trichiasis (normally located hairs abnormally directed on to the ocular surface). Older English cocker spaniels often suffer from concurrent keratoconjunctivitis sicca (KCS) and systemic hypothyroidism, in the author’s experience.
S
Figure 2. Left eye upper and lower distichiasis in a 14-week-old Labrador retriever. This patient had increased tear production and epiphora, but no actual keratitis and/or corneal ulceration.
pastic entropion – ocular pain causes retraction of the globe and contraction of the orbicularis oculi muscle, resulting in entropion – especially if the individual has an increased propensity to entropion; that is, overlong eyelid conformation.
Cicatricial entropion (least common) – eyelid scarring and distortion following injury and/or surgery results in eyelid distortion and entropion.
Treatment
Treatment options include:
Temporary eyelid tacking sutures – the author generally reserves temporary eversion of the eyelids via skin sutures for Shar Pei puppies only when they are between 8 and 16 weeks of age. Puppy entropion in other breeds of dog rarely self-correct in time; so, in the author’s experience, a permanent surgical solution is preferred.
Permanent surgical correction – the majority of dogs suffering from entropion have over-long eyelids. Therefore, a combination of eyelid shortening (eyelid wedge excision) and eyelid eversion (modified Hotz-Celsus procedure) forms the basis of the majority of entropion correction in dogs. A variation of this combination surgery has been described by Read and Broun (2007).
Some cases of breed-related entropion in dogs can prove complex, often requiring multiple surgical procedures. Managing the client’s expectations in such cases prior to surgical intervention is important and referral should be considered where appropriate. While a Stades procedure has been well documented at correcting senile entropion/excessive facial droop, the author favours an exaggerated upper modified Hotz-Celsus procedure +/− a rhytidectomy (facelift) if required.
Distichiasis
Distichiasis (Figure 2) is where extra eyelashes originate along the eyelid margin within or adjacent to the meibomian gland openings.
Clinical signs
Distichia normally cause clinical signs in younger dogs – that is, younger than 12 months of age. Clinical signs include:
increased tear production and epiphora
increased blink rate
ulcerative keratitis (position of the ulcer corresponds with the location of the distichia)
Causes
Causes of distichiasis include:
Breed related – the flat-coated retriever, bulldog, Staffordshire bull terrier, boxer, cavalier King Charles spaniel, miniature dachshund (long-haired), English cocker spaniel, pug and Pekingese, to name the most common.
Treatment
No one technique is 100% effective at resolving distichiasis, hence multiple options are available. These include:
Eyelid wedge excision – this is very effective if a single offending distichium or clump of distichia exists.
Transconjunctival thermal electrocautery (author’s choice) – a high temperature fine tip cautery is passed through the palpebral conjunctiva 4mm from the eyelid margin at the level of the distichium to a depth of 2mm and then immediately removed. The distichia are then plucked.
Cryotherapy – a rapid freeze and slow thaw (facilitated by a chalazion clamp) for two cycles damages the distichia follicles. This is good for dogs with thicker eyelids and multiple distichia, but can be associated with eyelid swelling and depigmentation. Iatrogenic damage to the meibomian glands can lead to qualitative tear film deficiencies in the long term. This is less effective if the cilia are non-pigmented.
Electrolysis – a time-consuming technique that can lead to scarring and distortion of the eyelids, especially in dogs with finer eyelids.
Sharp knife surgery – the follicles of the distichia can be excised en-bloc via a transconjunctival (palpebral) approach with the aid of a chalazion clamp and fine punch biopsy (2mm).
Ectopic cilia
Ectopic cilia (Figure 3) emerge through the palpebral conjunctival close to the eyelid margin and are directed perpendicularly to the corneal surface.
Clinical signs
Once erupted, ectopic cilia nearly always cause clinical signs. These include:
blepharospasm (relieved by the application of topical local anaesthetic solution)
increased tear production and epiphora
increased blink rate
ulcerative keratitis (position of the ulcer corresponds with the location of the ectopic cilium, usually in the middle of the upper eyelid)
Causes
Causes of ectopic cilia include:
Breed related – the flat-coated retriever, bulldog, shih-tzu and Pekingese, to name the most common.
Treatment
Treatment options include:
Surgical excision – the follicle of the ectopic cilium is excised en-bloc using a 2mm punch biopsy or 65 Beaver scalpel blade with the aid of a chalazion clamp. Additional local cryotherapy can also be used to treat the follicles of any unerupted cilia.
Conjunctivitis
Conjunctivitis (Figure 4) is a relatively common condition encountered in general practice and is usually secondary to other ocular or systemic disease processes in dogs.
Tear film deficiency (qualitative and/or quantitative).
Allergic disease.
Breed-related ocular conformation – doliocephalic breeds can develop “medial canthal pocket syndrome” whereby mucus and debris accumulate within the natural pockets, resulting in low-grade conjunctivitis.
Bacterial infection – secondary to another cause, such as KCS.
Viral infection – uncommon, but examples include canine distemper virus, canine herpesvirus-1 and canine adenovirus-2.
Ligneous conjunctivitis – a very unusual systemic disorder related to a plasminogen deficiency also affecting the oral, upper respiratory and urinary tract epithelium.
Neoplasia – primary conjunctival neoplasia is rare in dogs and usually benign (conjunctival melanoma being the exception). Conjunctival mast cell tumours, which are overrepresented by Labrador retrievers, can present with recurrent episodes of chemosis. Other primary conjunctival neoplasms include haemangioma/sarcoma, squamous cell carcinoma and papilloma.
Treatment
Address and treat the underlying cause. In cases of entropion, ectropion, trichiasis and eyelid agenesis, surgical intervention is warranted. If due to an underlying tear film deficiency, topical lacrimogenic and/or lacrimomimetic therapy should be considered.
Follicular conjunctivitis – a condition not uncommon in younger retriever-type dogs, presumably secondary to mild allergic disease – often spontaneously resolves with age, but can respond well to topical mast-cell stabilisers; for example, sodium cromoglycate. Other topical medical options for this condition include bromfenac and ciclosporin. The long-term use of topical glucocorticoids should be avoided due to the risks of associated corneal lipidosis.
If neoplasia is suspected then a snip biopsy or fine needle aspiration can be performed conscious following the application of topical local anaesthetic solution. As discussed, the majority of primary conjunctival tumours in dogs are benign and, therefore, surgical excision is recommended, although local recurrence is possible. Conjunctival mast cell tumours often do not recur even following incomplete excision in some cases.
KCS
KCS (Figure 5) is a common clinical disease that arises as a result of a deficiency of the aqueous component of the tear film being characterised by desiccation of conjunctiva and the cornea.
Clinical signs
Clinical signs include:
blepharospasm
conjunctival hyperaemia
tenacious mucopurulent ocular discharge
lacklustre appearance to the corneal surface
corneal neovascularisation
corneal pigmentation
progressive corneal ulceration
Causes
Causes of KCS include:
Immune-mediated (most common) – bilateral immune-mediated destruction of the lacrimal glands is the most common aetiology of KCS in our canine patients and certain breeds are overrepresented, including the West Highland white terrier, cavalier King Charles spaniel, English cocker spaniel and shih-tzu.
Neurogenic – neurogenic dry eye is when the parasympathetic innervation to the lacrimal glands is lost. This is usually a unilateral condition with the majority of cases having an ipsilateral dry nose (this is due to shared innervation of the tear gland and glands of the nasal planum on each side). In the absence of other concurrent neurological abnormalities – for example, facial nerve paralysis and/or Horner’s syndrome – these cases are typically idiopathic.
Endocrine disease – diabetes mellitus, hypothyroidism and hyperadrenocorticism have been linked to canine KCS.
Drug-induced – systemic sulphonamides and etodolac, topical atropine local anaesthetic solution and sedation/general anaesthetic.
Iatrogenic – surgical removal of the nictitans gland.
Infectious disease – distemper and leishmaniosis.
Evisceration/intrascleral prosthesis implantation – such dogs often develop KCS long term associated with reduced corneal sensation.
Local irradiation.
Congenital – the Yorkshire terrier, English cocker spaniel and cavalier King Charles spaniel (ichthyosiform dermatosis).
Treatment
Treatment options include:
Lacrimostimulants – topical ciclosporin achieves its action through both immunomodulating and tear stimulating properties. This calcineurin inhibitor blocks the activation and proliferation of T lymphocytes involved in immune-mediated lacrimal gland dysfunction. It also has an additional mucinogenic effect, which helps improve the quality of the pre-ocular tear film. A small amount of the drug should be applied to both eyes twice daily and it may take up to six weeks to exert its maximal beneficiary effects. Stronger concentrations of the drug can be compounded “in-house” with corn oil, but concentrations greater than 1% tend to cause local irritation, in the author’s experience.
Regarding topical tacrolimus, tacrolimus is a macrolide antibiotic that achieves its action in a similar way to ciclosporin A.
Oral pilocarpine eye drops 1% can be used to treat neurogenic, and some congenital, KCS cases. This parasympathomimetic agent is given by mouth at an initial dose of 1 drop/10kg two to three times daily and titrated to effect. The dose is gradually increased until a beneficial clinical effect is noted – that is, increased tear production. However, in poorly responsive cases the dose may have to be increased until signs of systemic toxicity are noted (hypersalivation, vomiting, diarrhoea and cardiac arrhythmias), at which point it is discontinued and restarted at a lower dose.
Lacrimomimetics – paraffin-based ointments coat and protect the corneal surface well, but can be more challenging for the client to apply.
Antibiotics – topical antibiotics with a broad spectrum of activity, such as chloramphenicol, may also be of benefit early on in the treatment course of canine KCS. Secondary bacterial infections are not infrequent in KCS due to inadequate cleansing of the ocular surface.
Surgical intervention – in medically refractive cases of canine KCS surgical intervention should be considered in the form of a parotid duct transposition. This surgery can be challenging and is associated with a relatively high postoperative complication rate, although case selection is very important.
Figure 3. Right eye upper ectopic cilium (pigmented) in a six-month-old cocker spaniel.
Figure 4. Left eye follicular conjunctivitis and deep-medial canthal pocket syndrome in a nine-month-oldflat-coated retriever.
Figure 5. Right eye chronic keratoconjunctivitis sicca in a seven-year-old cocker spaniel. Note the tenacious mucopurulent ocular discharge and corneal neovascularisation.
Indolent superficial ulcers (superficial chronic corneal epithelial defects; Figure 6) – typically persist for more than two weeks and are characterised by loose, non-adherent epithelial edges. As aforementioned, certain breeds are more likely to suffer from a superficial chronic corneal epithelial defects.
Clinical signs
Clinical signs include:
superficial corneal ulcer with loose, non-adherent epithelial edges
blepharospasm (these ulcers can be more painful than deeper lesions due to the more superficial distribution of the sensory nerves within the corneal surface)
conjunctival hyperaemia
ocular discharge (serous, mucoid, mucopurulent)
corneal neovascularisation
Causes
Causes of corneal ulceration include:
An inherent corneal defect – the pathophysiology is related to an abnormal, acellular hyaline zone in the superficial stroma. This layer prevents the overlying epithelial cells from forming adhesion complexes and, therefore, “sticking down” to the stroma and preventing the normal process of re-epithelialisation.
Treatment
Medical treatment alone is unlikely to be successful in such ulcers. Instead, treatment is aimed at disrupting the abnormal layer within the anterior stroma to allow epithelial attachment to the stroma. Possible treatments include:
debridement alone – associated with an approximately 50% healing rate
debridement and keratotomy (grid or punctate) – associated with an approximately 85% healing rate
diamond burr debridement – associated with an approximately 92% healing rate
superficial keratectomy – associated with an approximately 100% success rate
Irrespective of treatment, the corneal surface should always be aseptically prepared using dilute povidone-iodine solution (1 in 40 dilution) following the application of topical local anaesthetic solution. In addition, if using the corneal burrs, proper cleaning and sterilisation are paramount to prevent unwanted post-procedure infections.
Concurrent medical treatment should include a broad-spectrum topical antibiotic (for example, chlortetracycline hydrochloride) and systemic analgesia (for example, an oral NSAID). A bandage contact lens is also of benefit to the patient as it minimises postoperative ocular discomfort. The author uses topical ointments in combination with the lenses and, to date, has experienced no associated complications despite data sheet advice.
Corneal ulceration – progressive corneal ulcers
Progressive corneal ulcers (Figure 7) progress from being superficial to involve the deeper corneal stromal layers. This is due to active loss of the corneal stroma secondary to focal collagenolysis. Further progression can result in exposure of the Descemet’s membrane, leading to a descemetocele and subsequent corneal rupture.
Clinical signs
Clinical signs include:
Deeper corneal ulcer – focal indentation of the corneal surface.
“Halo” staining pattern of fluorescein (descemetocele) – the Descemet’s membrane does not take up the stain, whereas the collagen within the corneal stroma does.
“Intensive” staining pattern of fluorescein (keratomalacia) – fluorescein fluoresces more intensely using a cobalt blue light when the collagen is actively “melting”.
Blepharospasm – becoming less severe.
Conjunctival hyperaemia.
Ocular discharge – mucopurulent.
Corneal neovascularisation.
A reflex anterior uveitis – this reflex is more pronounced in brachycephalic dogs. If hypopyon is present, this does not mean infection exists within the globe, but represents the migration of white blood cells into the aqueous humour due to the uveitis and breakdown of the blood-ocular barrier.
Causes
Causes of corneal ulceration include:
Bacterial infection – Pseudomonas and Streptococcus species are most commonly involved.
Topical corticosteroids – with a pre-existing corneal ulcer.
Brachycephalic dog breeds – these types of dog appear much more prone to developing collagenolysis; therefore, appropriate treatment with ulcerative keratitis in any brachycephalic is very important (see further on).
Corneal cytology and culture/sensitivity should be performed in all progressive corneal ulcers, if finances allow. Treatment options include:
Anti-collagenases – topical serum (autologous or donor) is a good broad-spectrum anti-collagenase that is freely available. Other options include topical chlortetracycline hydrochloride and systemic doxycycline, but these are not as broad-a-spectrum anti-collagenase.
Antibiotics – a topical fluoroquinolone, such as ofloxacin, is appropriate for Pseudomonas species infection. Topical chloramphenicol is appropriate for Streptococcus species. The author uses these two drugs together in severe infections – chloramphenicol becomes bactericidal as a topical application in much higher concentrations; therefore, it can be used in combination with a fluoroquinolone that is also bactericidal. A broad-spectrum systemic antibiotic should also be used in such cases – for example, cephalexin – as well as appropriate systemic analgesia, for example, a systemic NSAID.
Surgical intervention – corneal cross-linking – a relatively new technology using a specific wavelength of UV light in combination with topical riboflavin – has been shown to halt collagenolysis, as well as induce new cross-links between the collagen fibres of the cornea. Once the aforementioned process has been performed, a lamellar corneoconjunctival transposition graft can be used to fill any resultant corneal defects, while maximising corneal transparency and vision.
Uveitis
Uveitis (Figure 8) refers to inflammation of the uveal tissue. Anterior uveitis is inflammation of the iris (iritis) and ciliary body (cyclitis); posterior uveitis is inflammation of the choroid. Panuveitis is inflammation of all three portions of the uvea.
Uveitis occurs when the immune privilege mechanisms for the eye become overwhelmed and the blood-ocular barriers break down. Uveitis can be caused by primary ocular disease or secondary to non-ocular disease.
Clinical signs
Clinical signs specific to uveitis include:
photophobia
aqueous flare
anterior chamber fibrin
keratic precipitates
hyphaema
hypopyon
iris swelling
rubeosis iridis (iris neovascularisation)
iris nodules
miosis
reduced intraocular pressure (IOP)
Clinical signs not specific to uveitis include:
corneal oedema
blepharospasm
epiphora
conjunctival and episcleral hyperaemia
decreased vision
Causes
The diagnosis of uveitis in dogs is relatively straightforward, but identifying the underlying cause can be unrewarding, mainly due to the relatively high incidence of idiopathic uveitis. Causes include:
drug-induced – for example, prostaglandin analogues
Treatment
Irrespective of the cause, both topical and systemic anti-inflammatory medications are required. Treatment options include:
Topical corticosteroids – for example, prednisolone acetate. These should only be used if the cornea is fluorescein negative.
Topical NSAIDs – for example, bromfenac. This type of drug, although not quite as potent as the corticosteroid, is preferred in chronic use due to the lack of associated side effects – for example, corneal lipidosis with chronic topical corticosteroid. Topical NSAIDs can be given in combination with a corticosteroid having a synergistic anti-inflammatory effect when used together.
Systemic corticosteroids – ideally, systemic corticosteroids should only be used once an underlying infectious cause to the uveitis has been ruled out. However, in severe cases of canine uveitis, immediate, immunosuppressive doses of systemic corticosteroids may be required to preserve vision (ideally, blood samples should be taken before the treatment is given). The dosage of oral corticosteroids can be gradually reduced and discontinued if the signs of uveitis become controlled. Often, a second immunomodulatory drug (see below) can be prescribed to prevent long-term recurrences of the ocular disease.
Systemic NSAIDs – these drugs are a safe alternative to systemic corticosteroids, especially before an underlying infectious cause has been ruled out. However, care should be taken in cases of gastrointestinal and/or renal disease. In addition, these drugs can affect platelet function.
Systemic immunomodulatory drugs – oral ciclosporin is the author’s choice as a long-term treatment option in cases of immune-mediated uveitis. This drug can be started at the same time as the oral corticosteroids, and then continued as the latter are reduced and discontinued.
Figure 6. Right eye spontaneous chronic corneal epithelial defects in an eight-year-old boxer. Note the under-running of the epithelial edges dorsally. This eye had undergone a previous grid keratotomy. The distichia are not significant.
Figure 7. Righteye progressivedeep stromal depthcorneal ulcer in aseven-year-old shih-tzu.
Figure 8.Right eye lens-induced uveitis in a seven-year-olddiabetic Labrador retriever.
Glaucoma
Glaucoma (Figure 9) is a complex of pathological events arising as a result of the elevation of IOP above normal limits. The earliest effect is on the optic nerve head and retina, leading to vision loss, which may rapidly become irreversible. In addition, glaucoma is a significant cause of pain, which can be difficult to control.
Clinical signs
Acute clinical signs include:
raised IOP (greater than 18mmHg to 20mmHg measured using a tonometer)
pain (blepharospasm, epiphora, head shyness, depression and anorexia)
episcleral/conjunctival congestion/hyperaemia
vision loss in the affected eye
corneal oedema
mydriasis
reduced direct pupillary light reflex (caused by iris sphincter muscle paralysis due to a high IOP)
Chronic clinical signs include:
pain reduces
globe enlarges (hydrophthalmos)
“Haab’s striae” (tears in Descemet’s membrane)
lens subluxation/luxation (as the globe enlarges, the lens zonules stretch)
“cupping” of the optic disc (posterior displacement of the optic nerve head)
optic nerve atrophy
retinal degeneration +/- detachment
intraocular haemorrhage
phthisis bulbi (end-stage)
Causes
Figure 9. Right eye acute primary closed angle glaucoma in a five-year-old basset hound.
Glaucoma is generally sub-divided into two major types – primary and secondary. Primary glaucoma is not associated with any other ocular pathology, while secondary glaucoma is the result of pre-existing ocular disease. Causes include:
Primary open angle (uncommon) – the drainage apparatus looks normal on light microscopy in the early stages of the condition, hence the term “open angle”. Breeds affected include the Shar Pei and Jack Russell terrier. Individuals affected often present late on in the disease process with bilateral enlarged globes, sometimes still visual.
Primary closed angle; goniodysgenesis (more common) – this breed-related disease results in abnormalities within the pectinate ligament affecting the drainage of the aqueous humour later in life. Breeds affected include the basset hound, flat-coated retriever, golden retriever, English springer spaniel, Welsh springer spaniel, cocker spaniel, Hungarian vizsla, Japanese shiba inu, Dandie Dinmont terrier, border collie, Leonberger, Spanish water dog and Siberian husky. Gonioscopy is performed on the non-glaucomatous eye to visualise the iridocorneal drainage angle to identify if goniodysgenesis is present.
Secondary to:
lens luxation – commonest in terrier breeds (note, chronic glaucoma can also cause lens luxation)
uveitis
neoplasia
abnormal pigment deposition (ocular melanosis in the cairn terrier)
intraocular haemorrhage
vitreous prolapse after intraocular surgery
fibrovascular membrane formation over pectinate ligament, aka pre-iridal fibrovascular membranes (chronic intraocular disease such as chronic uveitis, retinal detachment and neoplasia)
Treatment
Figure 10. Left eye immature nuclear cataracts in a two-year-old cocker spaniel. These lens changes were most likely congenital in combination with an abnormally small globe as part of a multiple ocular defect syndrome.
Acute glaucoma requires urgent medical management to reduce the IOP as soon as possible, and hopefully preserve optic nerve head function and vision. The use of topical medication has superseded systemic treatments due to their increased efficacy and reduced side effects.
The management of chronic glaucoma is aimed at reducing discomfort. Glaucoma secondary to uveitis requires additional treatment for the uveitis, as well as the high IOP (see aforementioned). Appropriate systemic analgesia should also be considered – especially in acute cases.
Some ophthalmologists also recommend systemic neuroprotective treatments to help maintain the optic nerve head function – for example, pimobendan – but the scientific evidence for the beneficial effects of these drugs in glaucoma is lacking. Treatment options include:
Topical prostaglandin analogues (first line treatment) – these drugs are very effective at lowering a very high IOP within 60 minutes. They also induce miosis, so are contraindicated in cases of anterior lens luxation. They can also worsen concurrent uveitis.
Travoprost – applied two to four times daily.
Latanoprost – applied two to four times daily.
Topical carbonic anhydrase inhibitors – these drugs are much less effective at lowering IOP and are better suited to secondary glaucoma. They can also be prescribed as a prophylactic medication for the fellow eye in cases of primary closed angle glaucoma and are synergetic when used in combination with prostaglandin analogues. Brinzolamide is better tolerated long-term due to their physiological pH.
Brinzolamide – applied three times daily.
T
Figure 11. Right eye nuclear sclerosis in a middle-aged Labrador retriever. Note the translucent rings visible within the lens.
opical combination treatments – these drug combinations have the addition of the beta blocker timolol, making them slightly more effective at lowering the IOP. Care should be taken with regards to systemic absorption in smaller patients.
travoprost + timolol
latanoprost + timolol
brinzolamide + timolol
Surgical intervention –
lentectomy (anterior primary lens luxation)
bypass surgery (gonioimplant surgery)
laser cyclophotocoagulation (endoscopic or transscleral): recent advances using a micropulse transscleral laser much earlier in the disease process is showing some promise
enucleation
evisceration/intrascleral prosthesis implantation
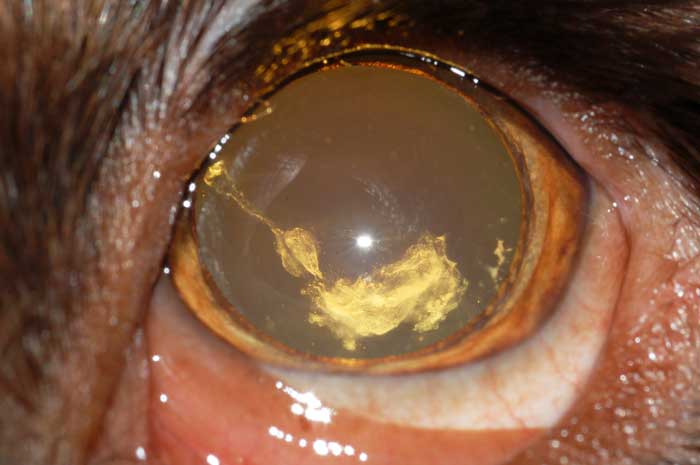
Cataracts
A cataract (Figures 10 and 11) is any opacity of the lens or lens capsule.
Clinical signs
Cataracts are described as:
incipient (less than 10% of lens involved)
immature (greater than 10% of lens, but tapetal reflex present)
mature (tapetal reflex not present)
hypermature (a “wrinkled” and irregular lens capsule)
Also, by their position within the lens:
capsular
subcapsular
nuclear
cortical
anterior/posterior
polar
Causes
Primary causes of cataracts include:
hereditary/breed-related
senile
Secondary causes include:
metabolic (diabetes mellitus)
nutritional
external trauma
intraocular disease
electrocution
radiation
Treatment
Treatment options include:
Surgical intervention.
Medical management of lens-induced uveitis: topical NSAIDs, such as bromfenac +/- a systemic NSAID. Owners who would not consider cataract surgery need to be informed of the possible complications associated with chronic lens-induced uveitis – for example, retinal detachment and glaucoma.
Acknowledgements
The author would like to thank Heidi Featherstone, Christine Heinrich and Peter Renwick for some of the photos used.

 Entropion (Figure 1) is inversion of the eyelid(s), resulting in contact of eyelid hairs with the ocular surface leading to irritation and corneal disease.
Entropion (Figure 1) is inversion of the eyelid(s), resulting in contact of eyelid hairs with the ocular surface leading to irritation and corneal disease.
 Distichiasis (Figure 2) is where extra eyelashes originate along the eyelid margin within or adjacent to the meibomian gland openings.
Distichiasis (Figure 2) is where extra eyelashes originate along the eyelid margin within or adjacent to the meibomian gland openings. Ectopic cilia (Figure 3) emerge through the palpebral conjunctival close to the eyelid margin and are directed perpendicularly to the corneal surface.
Ectopic cilia (Figure 3) emerge through the palpebral conjunctival close to the eyelid margin and are directed perpendicularly to the corneal surface. Conjunctivitis (Figure 4) is a relatively common condition encountered in general practice and is usually secondary to other ocular or systemic disease processes in dogs.
Conjunctivitis (Figure 4) is a relatively common condition encountered in general practice and is usually secondary to other ocular or systemic disease processes in dogs. KCS (Figure 5) is a common clinical disease that arises as a result of a deficiency of the aqueous component of the tear film being characterised by desiccation of conjunctiva and the cornea.
KCS (Figure 5) is a common clinical disease that arises as a result of a deficiency of the aqueous component of the tear film being characterised by desiccation of conjunctiva and the cornea.


 Clinical signs
Clinical signs Progressive corneal ulcers (Figure 7) progress from being superficial to involve the deeper corneal stromal layers. This is due to active loss of the corneal stroma secondary to focal collagenolysis. Further progression can result in exposure of the Descemet’s membrane, leading to a descemetocele and subsequent corneal rupture.
Progressive corneal ulcers (Figure 7) progress from being superficial to involve the deeper corneal stromal layers. This is due to active loss of the corneal stroma secondary to focal collagenolysis. Further progression can result in exposure of the Descemet’s membrane, leading to a descemetocele and subsequent corneal rupture. Uveitis occurs when the immune privilege mechanisms for the eye become overwhelmed and the blood-ocular barriers break down. Uveitis can be caused by primary ocular disease or secondary to non-ocular disease.
Uveitis occurs when the immune privilege mechanisms for the eye become overwhelmed and the blood-ocular barriers break down. Uveitis can be caused by primary ocular disease or secondary to non-ocular disease.


 Acute clinical signs include:
Acute clinical signs include: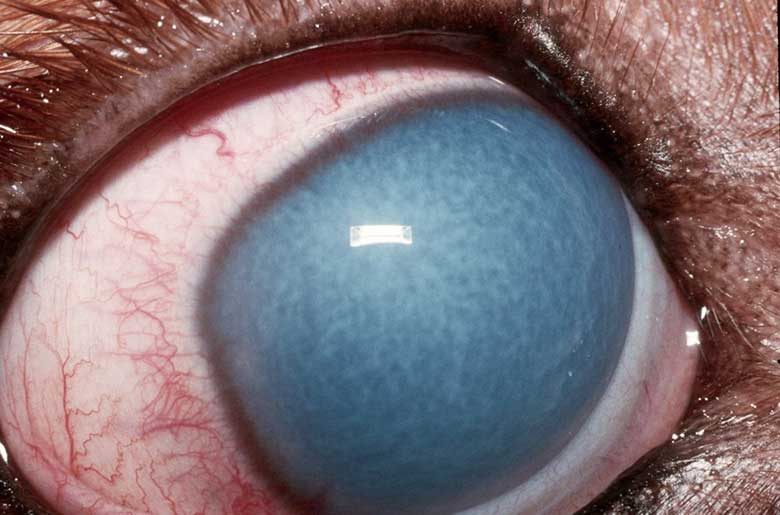

 Cataracts are described as:
Cataracts are described as: Secondary causes include:
Secondary causes include: