22 Apr 2019
Max Foreman recalls a feline presentation of a history of lethargy, inappetence and adipsia.
Max Foreman
Job Title
A four-year-old male, neutered domestic shorthair cat presented with a short history of lethargy, increasing inappetence and adipsia.

The owner also noticed the cat had been coughing for a few days, but had been very well and active prior to this. It had been vaccinated as a kitten, but had not seen a vet since its initial vaccinations, although it received intermittent flea and worming treatment.
On clinical examination, the cat was lethargic, moderately dehydrated (8%) and had a pyrexia at 40.4°C. Abdominal palpation was normal, as was thoracic auscultation.
Baseline haematology showed a stress leukogram, and biochemistry was all within normal limits.
Following rehydration with IV crystalloids, NSAIDs were given, to which no change occurred in the elevated temperature. Thoracic radiography showed a mild pleural effusion, which was confirmed on thoracic focused assessment with sonography for trauma.
Thoracocentesis and in-house cytology confirmed a pyothorax, and a unilateral low-profile thoracic drain was placed to allow full drainage and repeated flushing of the effusion.
Systemic antibiosis (co-amoxiclav 22mg/kg every 8 hours and metronidazole 10mg/kg every 12 hours) was started, and gave a rapid improvement in temperature, demeanour and appetite.
The drain was removed when no further fluid was aspirated, and the cat was discharged on a six-week course of antibiosis.
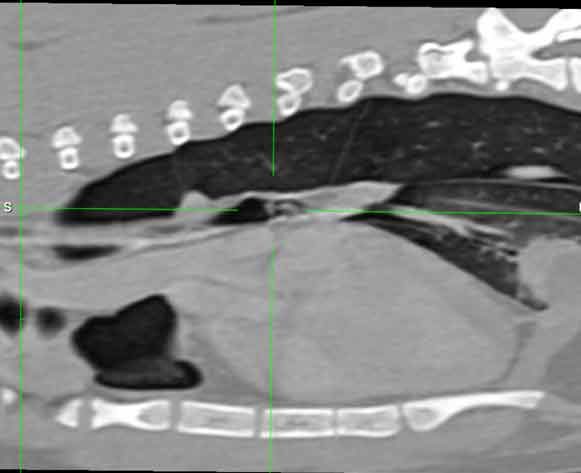
The cat had a continued good recovery; however, the owner noted an ongoing, although improved, intermittent cough. The decision was made to proceed with thoracic CT, which showed the presence of a bronchial foreign body.
Bronchoscopy was performed and used to remove a grass blade bronchial foreign body, which gave a complete resolution to clinical signs. The cat went on to make a full recovery.
This case is an example of non-penetrating bronchial foreign body as a cause of pyothorax in a cat.