17 Dec 2018
Alberto Palella Gómez recounts the presentation of a French bulldog with a cornea superficial ulcer that had been resistant to treatment.
Alberto Palella Gómez
Job Title
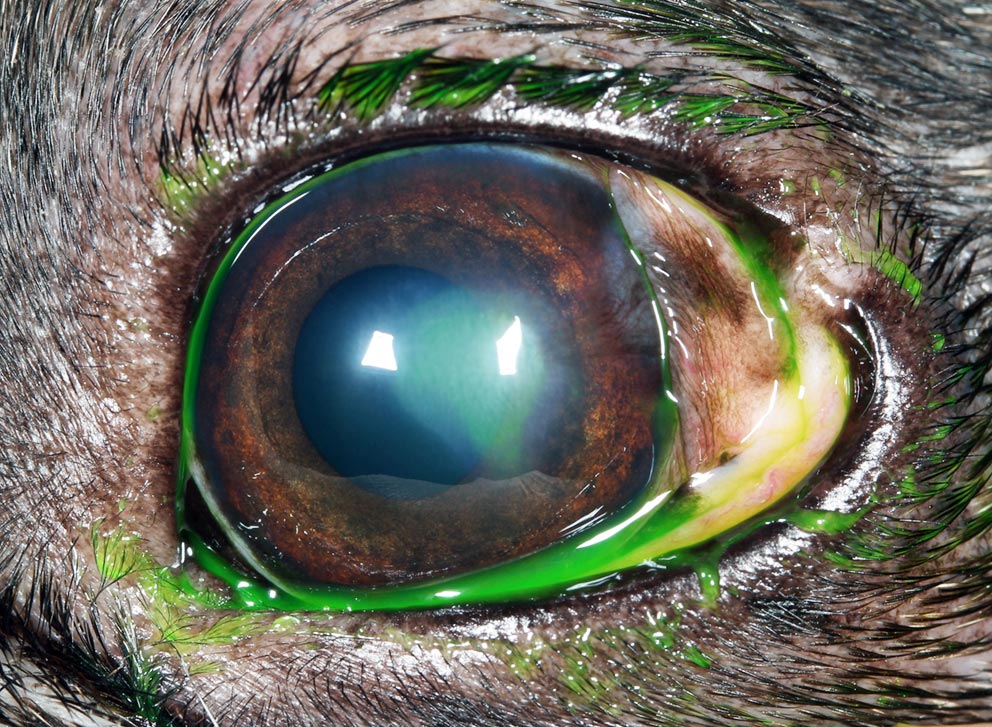
Figure 1. Note the moderate blepharospasm and mucopurlent discharge in the left eye.
Bella – an eight-year-old female, neutered French bulldog – has been diagnosed with a chronic superficial corneal ulcer (Figure 1) that has been refractory to medical treatment.
She was first presented to you with a two-week history of progressive ocular redness, mucopurulent discharge and mild to moderate discomfort of the left eye. Physical examination proved unremarkable and, apart from the ocular discomfort, Bella was a healthy dog with no previous history of eye problems.
After performing a complete ophthalmic examination, your clinical diagnosis is of a superficial corneal ulcer and you prescribe the following treatment:

A week after the initial visit, Bella is presented for re-examination, and you find the mucopurulent discharge has cleared and the conjunctival hyperaemia has reduced, but the ulcer is still present and slightly bigger.
However, this time you noticed something different – a ring of loose epithelium surrounding the corneal defect, resulting in a diffuse halo of less-intense fluorescein staining as the fluorescein diffuses underneath the poorly adherent epithelium (Figures 2a and 2b).
You have ruled out possible underlying causes for delayed corneal healing through a thorough examination, such as a foreign body, mechanical trauma, eyelid abnormalities (such as eyelid masses, entropion, distichiasis and ectopic cilia), tear film abnormalities (qualitative or quantitative deficits), facial nerve paralysis, exophthalmia or buphthalmia and severe corneal oedema.
What is your diagnosis? What treatment options would you recommend and what are their success rates?
After your ophthalmic examination on the second visit and ruling out all of the aforementioned differential diagnoses, you are confident you are dealing with a spontaneous chronic corneal epithelial defect (SCCED) – also known as an indolent ulcer, boxer ulcer or non-healing ulcer.
SCCEDs are chronic epithelial erosions that fail to resolve through normal corneal healing processes. The pathophysiology is not fully elucidated, but morphologic and functional abnormalities are described in dogs with this condition.
The epithelium surrounding the defect is poorly attached and exhibits dysmaturation, the basement membrane and adhesion complexes are normally absent or present in small discontinuous segments, and a thin superficial hyalinised acellular stromal zone composed of collagen fibrils admixed with amorphous fine fibrillary material is common (Bentley et al, 2001).
One important feature of SCCEDs is they are always superficial, with no stromal loss. Defects are found commonly in the axial or paraxial cornea, although any part of the cornea can be affected. Varying degrees of vascularisation may occur on up to 65% of cases (Bentley et al, 2001). The degree of blepharospasm varies between breeds, but tends to decrease with chronicity.
A SCCED diagnosis should be considered in middle-aged dogs with a superficial corneal ulcer when possible underlying causes have been ruled out and, despite medical treatment, no improvement has occurred within one to two weeks.
The client should be educated that treatment can be challenging, recurrence is possible and the contralateral eye could also become affected in the future.
Medical treatment alone is rarely successful at resolving SCCEDs, as underlying morphological and functional corneal abnormalities prevent the normal healing. Therefore, treatment options are aimed at disrupting these anomalies that preclude epithelial attachment to the stroma.
In a randomised, controlled clinical trial evaluating adjunctive tetracycline treatment in dogs with an SCCED (Chandler et al, 2010), dogs treated with topical oxytetracycline ophthalmic ointment, after manual debridement with a cotton-tipped applicator and grid keratotomy, healed significantly faster (74% healed within two weeks) compared to the control group (10% healed within two weeks) and dogs treated with oral doxycycline healed more rapidly than dogs in the control group, but the difference was not statistically significant.

It was hypothesised tetracyclines may be useful for the treatment of SCCEDs by upregulation of specific growth factors (for example, transforming growth factor beta and transcription factors) to promote corneal re-epithelialisation in dogs. It is important to highlight topical oxytetracyclines are not available for use in the UK.
The most common therapy for the treatment of SCCEDs is epithelial debridement. This can be used alone or in combination with other medical and surgical therapies.
Debridement after application of topical anaesthesia is usually performed with a dry cotton-tipped applicator. It is important to note normal epithelium cannot be removed with a cotton-tipped applicator, so debridement should be continued until only firmed adhered epithelium remains.
Typically, debridement can be repeated at 7-day to 14-day intervals. This procedure has an overall success rate of approximately 50% (Kirschner et al, 1991; Morgan and Abrams, 1994; Stanley et al, 1998).
Superficial multiple punctate keratotomy and grid keratotomy has been reported for the treatment of SCCEDs after epithelial debridement with a combined success of approximately 75% (Champagne and Munger, 1992; Morgan and Abrams, 1994; Stanley et al, 1998).
In a grid keratotomy, superficial linear incisions are made in a crosshatched pattern across the surface of the cornea using a 25G needle and extending approximately 1mm into unaffected surrounding cornea.
Superficial corneal debridement with a diamond burr (Figure 3) is also described and compared favourably to treatment with grid keratotomy, with 70% of cases healing after seven days and 92.5% of the cases at two weeks after debridement with diamond burr and application of a bandage contact lens (Davis and Gionfriddo, 2011; Sila et al, 2009; Gosling et al, 2013).
Although uncommon, 3% of dogs can develop keratomalacia as a complication, and buildup of contaminants on the diamond burr tip may be a contributing factor, therefore cleaning and sterilising the diamond burr tip is recommended (Spertus et al, 2017).
A bandage contact lens can be applied after all of the aforementioned procedures to improve comfort (Figure 4).

Superficial keratectomy has also been described as a treatment for SCCEDs by completely removing the abnormal superficial layer of stroma and allowing reformation of normal epithelial adhesion complexes.
Unlike the other procedures, the success rate is consistently 100% across studies, with corneal healing happening after one treatment in a median time of seven days.
This high success rate implies the stromal alterations are a critical part of the pathophysiology of the disease (Peiffer et al, 1976; Stanley et al, 1998).
When presented with a case of a chronic superficial corneal ulceration that is refractory to medical treatment, it is important to rule out any underlying causes, as aforementioned, for delayed corneal healing.
Once a diagnosis of SCCED has been made, and regardless of the technique used for its treatment, additional medical management with topical antibiotics (such as chloramphenicol), a systemic NSAID for the treatment of reflex uveitis (such as meloxicam), a topical cycloplegic to reduce the ciliary body muscle spasm (such as cyclopentolate), artificial tears (such as hyaluronic acid) and an Elizabethan collar to prevent self-trauma are required.
The author would like to thank Rodrigo Pinheiro de Lacerda and Samuela Mazzucchelli for their help reviewing this article. l Some drugs in this article are used under the cascade.