2 Jul 2018
Ariane Neuber describes how many differentials need to be excluded before a diagnosis of canine atopic dermatitis.
Ariane Neuber
Job Title
Allergic skin conditions are very common in dogs and cats, and can severely impede the patients’ and their owners’ quality of life.
Atopic dermatitis is defined as a pruritic, inflammatory dermatitis with characteristic clinical features that is genetically predisposed and often associated with IgE antibodies most commonly directed against environmental allergens (Halliwell, 2006). Diagnosis of atopic dermatitis occurs by excluding other differentials, which will be explored in detail in this article.
Many new therapies are available that can reliably be used to symptomatically treat the main symptom: pruritus; however, it is important to reach a diagnosis prior to committing to potentially lifelong therapy. A review by Hensel et al (2015) developed a set of practical guidelines based on a literature review of publications concerning the topic and is available as an open access publication.
If five criteria are fulfilled a sensitivity of 77.2% and specificity of 83% exists. If six criteria are fulfilled a sensitivity of 42% and specificity of 93.7% exists.
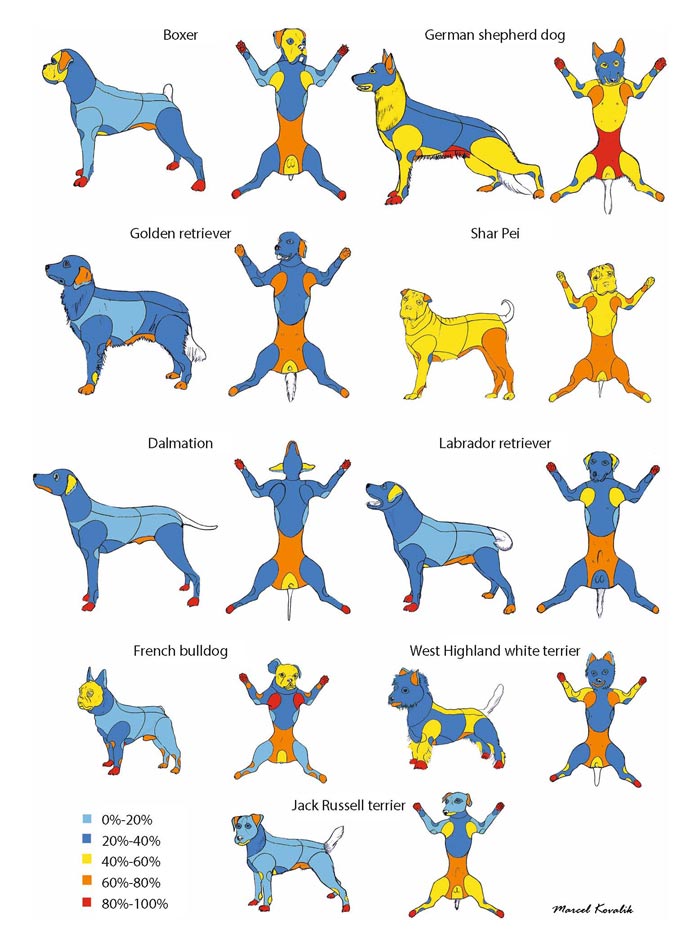
Canine atopic dermatitis (CAD) has got characteristic clinical features, although these are not pathognomonic and can vary immensely. This variation is possibly due to genetic variability, interbreed differences, inter-regional variation, individual variation, extent and chronicity of the lesions, the presence of flare factors, such as secondary infections, and concurrent diseases. Favrot et al (2010) published criteria for the clinical diagnosis of CAD (Panel 1).
Breed variation, in particular, can be enormous (Figure 1). Examples for breed-related phenotypes (Wilhem et al, 2011) include boxer dogs presenting with urticaria and/or otitis; French bulldogs with commonly affected eyelids, axilla and flexural surfaces; West Highland white terriers with yeast infections, oily seborrhoea and widespread disease; and German shepherds (Figure 2) with lesions on the elbows, thorax, hindlimbs, paws and groin. Contrary to the usual age bracket, in French bulldogs and Shar Peis the onset of disease is often below a year. The most common clinical signs are pruritus, otitis and recurrent infections, and manifestations thereof (for example, erythema, seborrhoea, alopecia due to self-trauma).
All pruritic diseases are potential differentials for CAD, with ectoparasites, cutaneous infections (which can be due to an allergic skin disease or other primary diseases; for example, an endocrine disease) and other allergies (adverse cutaneous food reaction, contact allergy or flea allergic dermatitis) most commonly seen.
In some cases, much rarer diseases, such as epitheliotropic cutaneous lymphoma, may be on the list of differential diagnoses. Scabies, in particular, can present in a very similar way to CAD. A thorough step-by-step approach is, therefore, needed to rule out other diseases reliably, rather than embark on lifelong symptomatic therapy before having made a diagnosis of a lifelong disease (CAD). Allergy testing is not useful as a screening test in pruritic dermatoses, as CAD is a diagnosis of exclusion.
Once parasites and infections – or, in selected cases, other causes – have been ruled out, it is important to identify the allergic trigger. Food can be a trigger for allergic individuals and a diet trial is the best way to determine whether food is implicated (Panel 2). A critically appraised review on cutaneous adverse food reactions (CAFR) of companion animals on the duration of elimination diets (Olivry et al, 2015) found that for diagnosing CAFRs in more than 90 per cent of dogs and cats, elimination diet trials should last at least eight weeks. A diet trial can only be assessed once parasites and infections have already been ruled out.
Parasites are commonly found on small animals and the clinical presentation can be very similar to allergic skin disease. It is, therefore, very important to investigate the possibility of parasites before diagnosing an allergy.
Fleas are common in many geographical areas. It is, therefore, imperative to rule out this differential thoroughly. Modern flea control methods are becoming more reliable in doing just that. However, a lack of understanding flea biology, exaggerated owner expectations of what a product can realistically achieve (rather than a resistance being present) and shortcomings in administering products in terms of frequency, lack of use on all in-contact animals (for example, doggy day care or unaffected pets in the same household), lack of environmental flea control and a high environmental burden (such as a garden, due to wildlife or roaming cats), can lead to a false sense of security and ruling out fleas inappropriately.
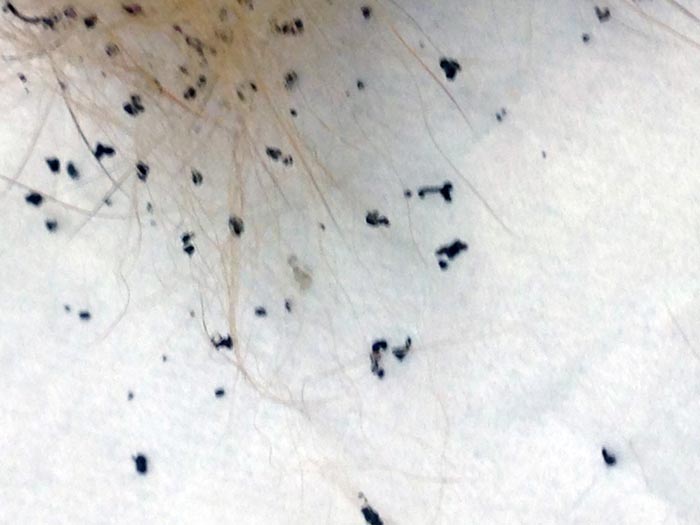
Fleas can be troublesome simply due to their presence (Figures 3 and 4) as a flea burden. They can cause flea allergic dermatitis (FAD) – when only a small number of bites cause a disproportionate level of pruritus (Figure 5) due to the host reaction – and they
are an important flare factor in pets suffering from another allergy. Fleas can also transmit several other diseases, such as tape worms.
It may be possible to find evidence of fleas on the patient; however, the lack of live fleas or flea dirt cannot be used to rule out this possibility conclusively. Flea infestation is associated with a flea burden; however, FAD is often characterised by a distinct lack of fleas on the patient, due to the severe irritation. Lesion location is usually on the tail base, lumbosacral area and the caudomedial thighs. Fleas can also be flare factors for patients with other allergies, including CAD, and it is possible for a dog with CAD to also have FAD.
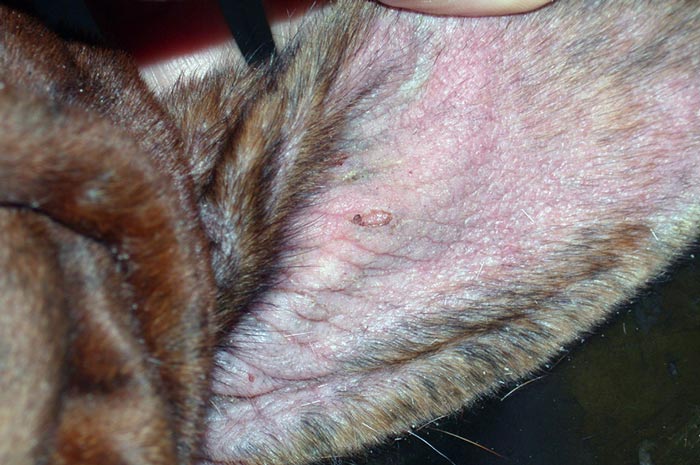
Scabies is usually an intensely pruritic dermatitis caused by infestation with Sarcoptes scabiei. This highly contagious mite can affect other dogs and foxes, and is also zoonotic. Many modern flea control products are reliably miticidal, so thorough flea control can, in many cases, eliminate this differential at the same time.
This condition often has a characteristic lesion distribution (pinnae, elbows and hocks; Figures 6 and 7) and, in many cases, a more acute onset of intense pruritus; however, quite a spectrum of history and clinical signs exist at presentation, and distinction by these features alone cannot be made.
Laboratory tests useful in the diagnosis of scabies (Neuber and Nuttal, 2017) are superficial skin scrapings (it is advisable to take numerous scrapings) and sarcoptic IgG ELISA. Occasionally, the mites can also be seen on biopsy or faecal flotation, but the former is certainly not reliable and far too invasive to be used for routine diagnosis.
If the clinical suspicion is high, and none of the laboratory tests are positive, treatment trials are indicated. The pinnal-pedal reflex is said to be indicative, although other diseases causing pinnal lesions can also cause a positive reflex. House dust mite allergens and Sarcoptes mites can cross-react on ELISA testing, and trial therapy is essential to rule out scabies prior to embarking on treatment for CAD.




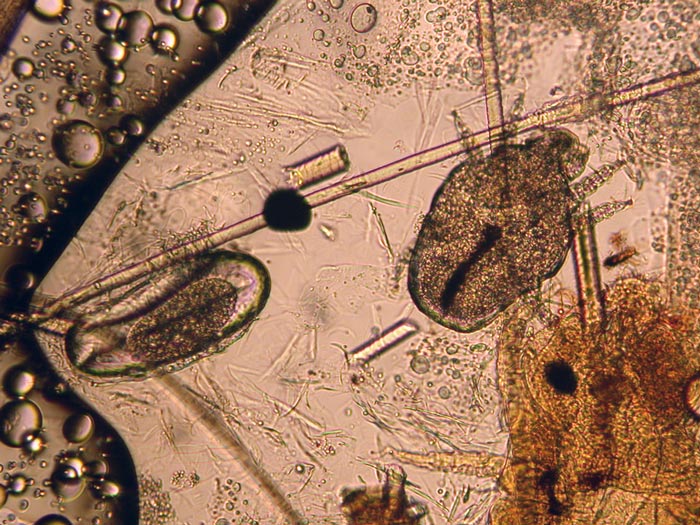
Other parasites, such as Demodex species, Otodectes cynotis, Cheyletiella species (Figure 8), lice or Neotrombicula autumnalis (harvest mites), can also mimic aspects of CAD, or act as flare factors. These are usually found in certain body regions:
These should be more readily found, with various methods available for the investigation of parasites than cases of sarcoptic mange, as they are usually present in higher numbers. Particularly useful methods to detect different species are (Figure 9):
Cutaneous infections are a common secondary feature of allergic (and other) skin disease and are often pruritic in their own right. They are, therefore, a major flare factor and can significantly change the clinical presentation of the underlying disease. Most common organisms involved in cutaneous infections are either Staphylococci or Malassezia.
Staphylococcus pseudintermedius is a normal resident on canine skin and the most common organism implicated in bacterial pyoderma in dogs. The clinical appearance varies a lot, with epidermal collarettes, pustules, alopecia, papules, crusts, scaling, erythema and pruritus all commonly seen. Diagnosis is usually made by combining the history, clinical appearance and performing cytology (Figure 10), which should show neutrophils, often degenerate and/or with intracellular cocci, possible macrophages and extracellular cocci.
Most cases of superficial pyoderma respond well to topical therapy alone. Shampoos, sprays, mousses, gels or wipes are commonly used. The choice of product depends on lesion distribution and spread, and owner preference. If the prevalence of multiresistant, often meticillin-resistant, staphylococci is high in the region, or if a history of repeated antibiotic use exists – or the condition is non-responsive to antibiotic use, despite the choice of an appropriate antibiotic for a long enough time at a sensible dose and compliance is good – a culture should be performed.
Patients should be re-evaluated after two weeks of treatment and at the end of the treatment course to ensure complete resolution of the clinical signs, as well as assessing the patient to identify the underlying disease to avoid future episodes of pyoderma. Further tests may be required at that stage, such as allergy testing or endocrine assays.

Malassezia pachydermatis is the most common yeast found on canine skin and is frequently involved in inflammatory dermatitides in dogs with a primary skin disease. Similar to staphylococcal pyoderma, patients with Malassezia dermatitis show a slightly changed clinical picture, and identification of their primary disease should be done after successful treatment of the yeast dermatitis.
Clinical signs include erythema, pruritus, greasy seborrhoea, greasy scaling and malodour. The organisms are usually readily identified on cytology, although some patients suffer from a Malassezia hypersensitivity and only small numbers of the yeast can trigger substantial pathology.
Cytologically, the yeast appears as a classical footprint, snowman or Russian doll-shaped budding yeast. Often, the yeast is found in the absence of inflammatory cells; however, occasionally, particularly in some cases of otitis, a neutrophilic inflammation can be seen. Culture is less reliable as false positive and false negative results can occur.
Cytology is an affordable and rapid diagnostic tool for this condition, and should be performed in all patients with compatible clinical signs. Topical therapy is usually very useful; however, in patients with Malassezia hypersensitivity, when small numbers of the organism elicit a disproportionate inflammatory response, systemic treatments may be needed to achieve adequate control.
Epitheliotropic cutaneous lymphoma can present with pruritus, and biopsy is the diagnostic tool of choice if it is suspected the patient may suffer from it.
A number of diseases need to be ruled out before a diagnosis of CAD can be made. Allergy testing becomes a useful tool once this has been done and its function is to identify the offending allergens. Allergy testing, however, is not useful as a screening test; it is merely a way to identify the allergens to perform allergen-specific immunotherapy or to practise allergen avoidance.
Most common differentials that need to be ruled out are parasites or infections. A logical, step-by-step approach is the best way of working up patients with pruritic skin disease.