14 Sept 2015
Christine Heinrich
Job Title
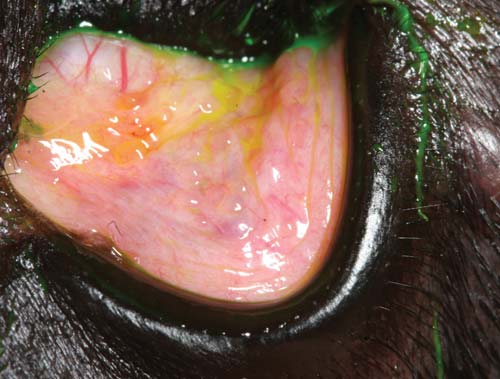
Figure 5a. Serous conjunctivitis in a Labrador retriever with canine atopic dermatitis. Up to 60% of patients with this condition show ocular signs of the disease, with conjunctivitis being the most prominent.
One would think making a diagnosis of conjunctivitis and treating it appropriately would be one of the easiest things to face in general practice. However, this is a misconception for a number of reasons.
Firstly, the conjunctivitis might merely be the presenting sign of another ocular condition, which will go unnoticed unless the examiner carefully searches for other clues and addresses the real ocular condition masquerading as conjunctivitis.
This is especially the case in canine patients, where there are very few “primary” forms of conjunctivitis and where true infectious conjunctivitis is rare.
In cats, primary conjunctivitis is more common, but the frustration is, even with the correct diagnosis, it might be difficult to cure the condition. The reason is feline patients may remain lifelong carriers of the organism causing their conjunctivitis (for example, with feline herpesvirus 1) or immunity against the organism may be short lived (for example, in chlamydial infections) and treatment for the condition may not only be required for the individual affected, but for all in-contact cats to prevent reinfection.
For practical reasons, this article will therefore address canine and feline conjunctivitis separately – to help provide practical guidelines in how to approach a canine versus a feline conjunctivitis case. However, we need a brief overview of anatomy and function of the conjunctiva to understand why conjunctivitis is such a common clinical sign in many ocular diseases.
The conjunctiva is the mucous membrane that covers the inner aspects of the eyelids and the scleral aspects of the globe. On the lid margin, the conjunctiva joins the eyelid skin at the mucocutaneous junction of the “grey line”, which is denoted by the Meibomian gland openings, and on the bulbar aspect, the conjunctiva inserts at the limbus. Only small amounts of conjunctiva are exposed in the normal dog eye and in the cat, the lids might have to be manipulated to allow visualisation of the conjunctiva (Figures 1 and 2). On the palpebral surface, the conjunctiva is tightly adherent to the lids while it overlies the bulbar aspect loosely.


As the most exposed mucous membrane in the body, the conjunctiva is highly vascular with lymphoid drainage and it contains a very active immune system termed the “conjunctiva-associated-lymphoid-tissue”, whose structure has been compared with an everted lymph node. The conjunctiva is an integral part of the ocular surface and thus inextricably linked with the precorneal tear film (PCTF).
Any deficiencies or abnormalities of either will have serious repercussions on the other. For example, the conjunctival goblet cells form the mucin component of the tear film – which, in a simplified model of the tear film, is required to “adhere” the tear film on to the corneal surface. A reduction in conjunctival goblet cells, such as reported in diabetic patients or in patients with chronic keratoconjunctivitis sicca (KCS), will result in reduced tear film stability (as can be measured by the tear film break-up time) and potentially secondary corneal disease (Cullen et al, 2005).
Vice versa, a reduction in the aqueous component of the PCTF will have a serious impact on conjunctival health and manifests as conjunctival hyperaemia, hyperplasia, keratinisation of the surface epithelium and ocular discharge.
The conjunctiva is richly vascularised with branching vessels, which explains the bright pink or red appearance it can take on when inflamed (Figure 3). At times, it might be helpful to distinguish the conjunctival vessels, which are freely mobile with the conjunctiva, from the underlying, fixed episcleral and scleral vessels. As a rule of thumb these are straighter, thicker and darker in appearance (Figure 4). When 2.5% phenylephrine is applied to the eye, conjunctival vessels are meant to bleach more rapidly and completely than the episcleral vessels.


The conjunctival surfaces are not sterile and several studies have described the “normal” bacterial flora in both cats and dogs, which varies with geographic location and season. In dogs, studies have reported positive bacterial cultures in 39% to 87% of normal patients with more than two-thirds of the isolates being Gram-positive (Gould and Papasoutiotis, 2013). In cats, bacteria have been isolated from the conjunctival sac of 4% to 67% of normal animals, again with the majority being Gram-positive (Gould and Papasoutiotis, 2013). The normal commensal conjunctival flora can easily be disturbed due to indiscriminate antibiotic use or in many chronic disease processes such as KCS.
Conjunctivitis describes the inflammation of the conjunctival membranes, which presents clinically with hyperaemia and discharge. Systems to classify conjunctivitis in textbooks include aetiological, according to the form of discharge or duration. When looking at the discharge in conjunctivitis, serous, mucoid and purulent are distinguished (Figures 5a to 5c).



Of course, the most helpful way to classify conjunctivitis would be according to its aetiology – including infectious (viral, bacterial, parasitic and fungal), allergic, toxic, associated with a PCTF deficiency or due to adnexal disease. Such an aetiological diagnosis is not always possible clinically as the clinical appearance can be very non-specific. Ulcerative or proliferative forms of conjunctivitis are rare, but may be a very specific indicator for certain diseases, unlike serous or purulent forms of conjunctivitis. Overall, it must be remembered conjunctivitis may be a non-specific clinical sign accompanying both ocular surface and intraocular conditions – including keratitis, uveitis and glaucoma.
Primary infectious conjunctivitis is rare in dogs (Hendrix, 2013) and the safest starting point is to assume the conjunctival inflammation is caused by another underlying disease. Only after exclusion of any other contributing factors should it be considered a canine patient might be suffering from an allergic or infectious form of conjunctivitis. A full ophthalmic and general examination of every canine patient presenting with conjunctivitis must be carried out and the key points to assess include:

KCS is one of the most common causes of conjunctivitis in dogs. Most patients with KCS that present with conjunctivitis will show tenacious mucoid or mucopurulent discharge (Figure 6).
Patients presenting with conjunctivitis and Schirmer tear test (STT) readings below 15mm of wetting/minute are highly suspicious to be suffering from KCS and correction of the tear production with appropriate medication (in most cases canine KCS will be responsive to cyclosporine in form of the licensed ciclosporin ointment, Optimmune) will result in resolution of the conjunctivitis.
Interestingly, patients with KCS have been reported to have a “changed” bacterial flora and while use of concurrent topical antibacterial medication in KCS management is acceptable, it is frequently found all signs of conjunctivitis resolve following restoration of tear production with topical ciclosporin even without antibiotic use. However, in severe cases of KCS, increased numbers of Pseudomonas have been cultured and appropriate topical antibiosis is indicated alongside aetiological treatment of the tear deficiency.
One newer thought is our canine patients may be suffering from KCS even before their STT readings are reduced to below 15mm of wetting/minute as it might be the quality of the tear film that deteriorates before the actual aqueous tear component is found reduced (Moore and Collier, 1990). Such patients frequently present in referral practice with signs of conjunctivitis, mild ocular irritation and epiphora, and sometimes even recurring corneal ulceration without any other obvious cause. The apparent epiphora (often taken as the key sign of conjunctivitis) is likely to be caused by poor tear film stability and “spilling over” of tears due to deficiencies in mucin or lipid layers of the PCTF.
Further clinical tests, such as the tear film break-up time (TBUT), may help diagnosis and the “diagnostic” use of ciclosporin may help confirm a diagnosis of “qualitative” KCS and result in resolution of the conjunctivitis (Heinrich, 2014).
A poor fit of eyelid-to-globe apposition often causes chronic conjunctival irritation and may present as conjunctivitis. This is especially the case in the following groups of patients:
It is, therefore, essential to assess the eyelid-to-globe apposition in any dog presenting with conjunctivitis. Ideally, this is first done “hands off” to prevent any reflex eyelid closure by the patient, which would make a spastic conformational problem worse or even impossible to detect as the patient shuts the affected eye.
Secondly, it is important to assess the patient’s eyelid position in the way it normally carries its head. This means for an ageing cocker spaniel, the patient must not sit on the consulting table with the head elevated, when the heavy facial brow would “slip backwards” and temporarily alleviate any trichiasis.
Instead, the eyelid opening is observed while the patient holds its nose low, which is how it would spend most of the day and when any facial droop and secondary trichiasis would become visible. To this purpose, the examiner might be required to kneel in front of the consulting table with the patient looking down.
Trichiasis, especially, can give rise to signs of conjunctivitis even before the lashes touch the cornea. In many patients with droopy upper lids, the lashes become trapped in the ventral conjunctival fornix during low head posture, where they have a wicking effect, resulting in epiphora, and cause chronic conjunctival irritation (Figures 7a and 7b). Chronic mechanical irritation by distichia or ectopic cilia can result in conjunctivitis, but often also shows as corneal disease (Figure 8).



Surgical correction of the abnormal eyelid position or removal of aberrant eyelashes will usually result in resolution of signs of conjunctivitis.
A careful search for conjunctival foreign bodies should be carried out in any patient presenting with conjunctivitis after STT readings have been obtained (Figure 9). It might be necessary to apply local anaesthestic to allow assessment of the conjunctival fornices, which can be explored with a cotton bud. The third eyelid might need to be lifted up and pulled out with a pair of blunt forceps. There is nothing more embarrassing than missing a grass seed that has become wedged behind the third eyelid.

Nasolacrimal drainage should be assessed to see whether epiphora is being misdiagnosed as conjunctivitis. Conjunctivitis can, of course, also be due to infection of the nasolacrimal system (Figure 10). A dog presenting with tear overflow in one eye, but without any signs of ocular irritation, might simply be suffering from absent nasolacrimal duct function on the affected side rather than from true conjunctivitis.
To assess the nasolacrimal drainage, a Seidel test is carried out. In this test, a generous amount of fluorescein is applied to both eyes and the appearance of the dye at the nostrils examined (Heinrich, 2014). The test is not always diagnostic as many dogs do not only have a nasal ostium of the duct, but additional openings in the oropharynx and the fluorescein may travel to the throat rather than the nose. However, if the dye shows up in the nostril on the unaffected side, but not on the affected side, this is highly likely to indicate a problem nasolacrimal duct function.
The conjunctiva is closely related to deeper ocular structures as both conjunctival and ciliary blood vessels at the limbal arcades communicate. This explains why the conjunctiva is involved in many other ocular conditions and why conjunctivitis can be such a universal presenting sign.
For example, in chronic corneal disease, budding conjunctival blood vessels, which lie superficially at the limbus, may give rise to superficial corneal blood vessels, while deep corneal vascularisation originates from the ciliary vessels at the limbus, which lie beneath the conjunctival vascular arcades. Both superficial and deep vessels at the scleral side of the limbus can be injected in many forms of ocular disease and, while theoretically it can be attempted, to distinguish the vessels being injected with the hope this might point towards the ocular structure being diseased, this is not always easy in practice.

Also, clinically conjunctival and ciliary injection is often concurrent (Figure 11). Conjunctivitis can, therefore, be a presenting sign in conditions as different as keratitis, uveitis and glaucoma, and a careful examination of the intraocular structures for any anomalies is indicated before a diagnosis of “simple conjunctivitis” is made.
One helpful hint in distinguishing conjunctivitis from KCS, adnexal disease, keratitis and intraocular disease is the latter are more likely to be associated with pain than a primary bacterial or allergic conjunctivitis. Patients presenting with conjunctivitis and significant ocular discomfort (blepharospasm, photophobia, reluctance to have eye or side of the face touched) must, therefore, be very carefully assessed to identify the underlying problem.
Signs that might particularly indicate a serious intraocular disease in a patient presented with conjunctivitis include:
Symptomatic treatment for a presumed allergic or bacterial conjunctivitis is not recommended if any of these have been identified as this might seriously delay diagnosis and appropriate treatment of the real and potentially painful and vision-threatening disease.
Once KCS, adnexal anomalies and other, potentially more serious, underlying ocular conditions have been ruled out, allergic, autoimmune-mediated or primary infectious conjunctivitis can be considered.

Allergic conjunctivitis is poorly understood in dogs and there is a dearth of insightful articles about the condition.
In most cases of allergic conjunctivitis, conjunctival hyperaemia and epiphora with only mild ocular irritation are seen (Lourenco-Martins et al, 2011). Affected patients are reported to “rub at their face” on occasions and STT readings are usually high.
A clear link to canine atopy has been made and, certainly, individuals affected with severe atopic dermatitis will present with extensive atopic blepharitis and concurrent conjunctivitis (Figure 12). These patients may show more obvious signs of irritation and a tendency to self-traumatise their face due to the blepharitis.
It is not clear whether the conjunctivitis is the only presenting sign in some patients suffering from canine atopy where no skin lesions are found. The use of a conjunctival provocation test to confirm allergic conjunctivitis in atopic canine patients has been described, but, to the author’s knowledge, it is not commercially available in the UK (Lourenco-Martins et al, 2011).
Conjunctival cytology or histology can be employed to confirm allergic conjunctivitis and the finding of eosinophils should raise a high suspicion index. Conjunctival scrapes are taken in the conscious patient under local anaesthesia by gently scraping across the conjunctiva in the dorsal or ventral fornix with the blunt end of a scalpel handle or with a cytobrush. Conjunctival biopsies are readily carried out after the repeat application of proxymetacaine eye drops (Minims proxymetacaine) by lifting the conjunctiva where it is loosely overlying the dorsolateral sclera and “snipping” off a small (3mm × 3mm) piece with sharp, rounded sterile scissors (Mitchell and Oliver, 2015).
Treatment of canine allergic conjunctivitis is usually symptomatic and carried out in relation to the severity of the clinical signs. In some patients, no treatment is required if conjunctival hyperaemia and epiphora are mainly of cosmetic concern.
However, if the patient shows signs of ocular discomfort then the use of topical steroids is indicated. Often, an initially high frequency of application of a prednisolone-acetate formulation or dexamethasone-containing eye drops may help to resolve clinical signs and long-term treatment is then reduced to the lowest possible maintenance level.
The use of topical mast-cell stabilisers has not been critically evaluated in canine allergic conjunctivitis and the efficiency of systemic antihistamines is also variable and not well documented. In patients where the conjunctivitis is part of a more severe form of systemic atopic dermatitis, systemic treatment with steroids, ciclosporin or Janus kinase inhibitors may also reduce the ocular signs.
Follicular conjunctivitis is believed to be due to chronic antigenic stimulation, but its relationship to allergic conjunctivitis is not clear and peer-reviewed reports on this topic are lacking.
This type of conjunctivitis is especially seen in young (less than 18 months of age) large breed dogs and those with deep conjunctival fornices appear to be predisposed.
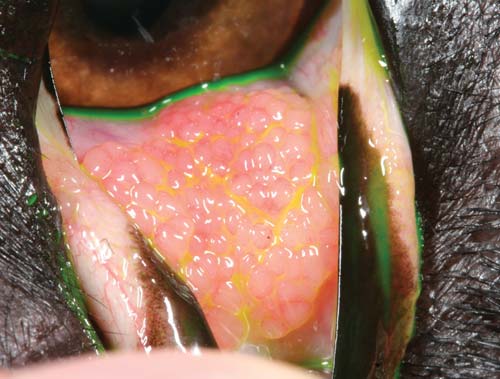
Affected patients present with mucoid to purulent ocular discharge and conjunctival hyperaemia. Close examination reveals the presence of multiple follicles, which are especially visible in the ventral conjunctival fornix and on the palpebral aspect of the third eyelid (Figure 13a). On occasions, marked follicle formation can also be seen on the posterior aspect of the third eyelid (Figure 13b).
Again, treatment is given according to how much the clinical signs are distressing patient or owner. Benign neglect is an acceptable way to manage mild forms of this condition. However, in some patients significant discharge or ocular irritation are observed and again, the use of topical steroids as for atopic conjunctivitis is indicated once all other causes of conjunctivitis have been ruled out.
The use of false tears and lacrimogenics has been recommended in the hope this will “flush out” the conjunctival fornices and reduce antigenic stimulation. Manual debridement of the follicles has been reported in the past, but techniques such as scarification or cautery of the follicles on the posterior aspect of the third eyelid should be discouraged, given the ductules of the third eyelid gland open into the same area of the posterior aspect of the third eyelid.

Lymphoplasmacytic infiltration of the third eyelid (also known as pannus) is characterised by mucopurulent discharge, depigmentation and thickening of the third eyelids (Figure 14). Affected patients are often presented by their owners as the eyes are perceived as “sore” in appearance – but, interestingly, the condition is only associated with very minor irritation for the patient and the sore appearance is based on the red and swollen third eyelids. The condition can occur concurrent with chronic superficial keratoconjunctivitis and both are believed to be due to an autoimmune mechanism.
Lifelong treatment is required to control the disease and following initial intensive treatment with topical steroids such as prednisolone-acetate up to six times daily, it is often possible to manage the disease long term with topical ciclosporin without or with low-frequency topical steroids.
As stated, primary infectious conjunctivitis in dogs is rare. Canine distemper virus can certainly cause serous to purulent conjunctivitis in the acute phase and KCS long term, but the disease is rare in the UK thanks to high vaccination uptake.
Canine herpesvirus infection has also been reported as a primary cause of canine conjunctivitis, but, from an ophthalmologist’s view, reports of this condition manifesting solely as conjunctivitis are largely limited to an experimental setting.
It has been suggested neonatal conjunctivitis is the result of transfer of this infection from dam to puppy during birth. Bacterial conjunctivitis is a possibility, but, in the author’s experience, is exceedingly rare, with most cases of persistent bacterial infection presented in practice associated with nasolacrimal duct disease. After exclusion of any possible underlying/concurrent ocular disease, sample for bacteriological culture and cytology should be obtained in patients with persistent conjunctivitis and forwarded for analysis so appropriate antibiosis can be given.
Failure to identify bacterial infection in suspicious cases or failure to respond to appropriate topical antibiosis should be seen as an incentive to refer the patient for assessment by an ophthalmic specialist – to ensure the true underlying cause has not been missed.