8 Mar 2022
Fergus Allerton BSc, BVSc, CertSAM, DipECVIM-CA, MRCVS explores the search for the optimal length of medication for UTIs in dogs.
Fergus Allerton
Job Title
Figure 1. Infographic provided to participating veterinarians outlining key time points in the SOS study (published in BMC Veterinary Research).
Multiple resources have been developed to raise awareness, and support measures, to mitigate the threat to human and animal health posed by antimicrobial resistance (AMR).
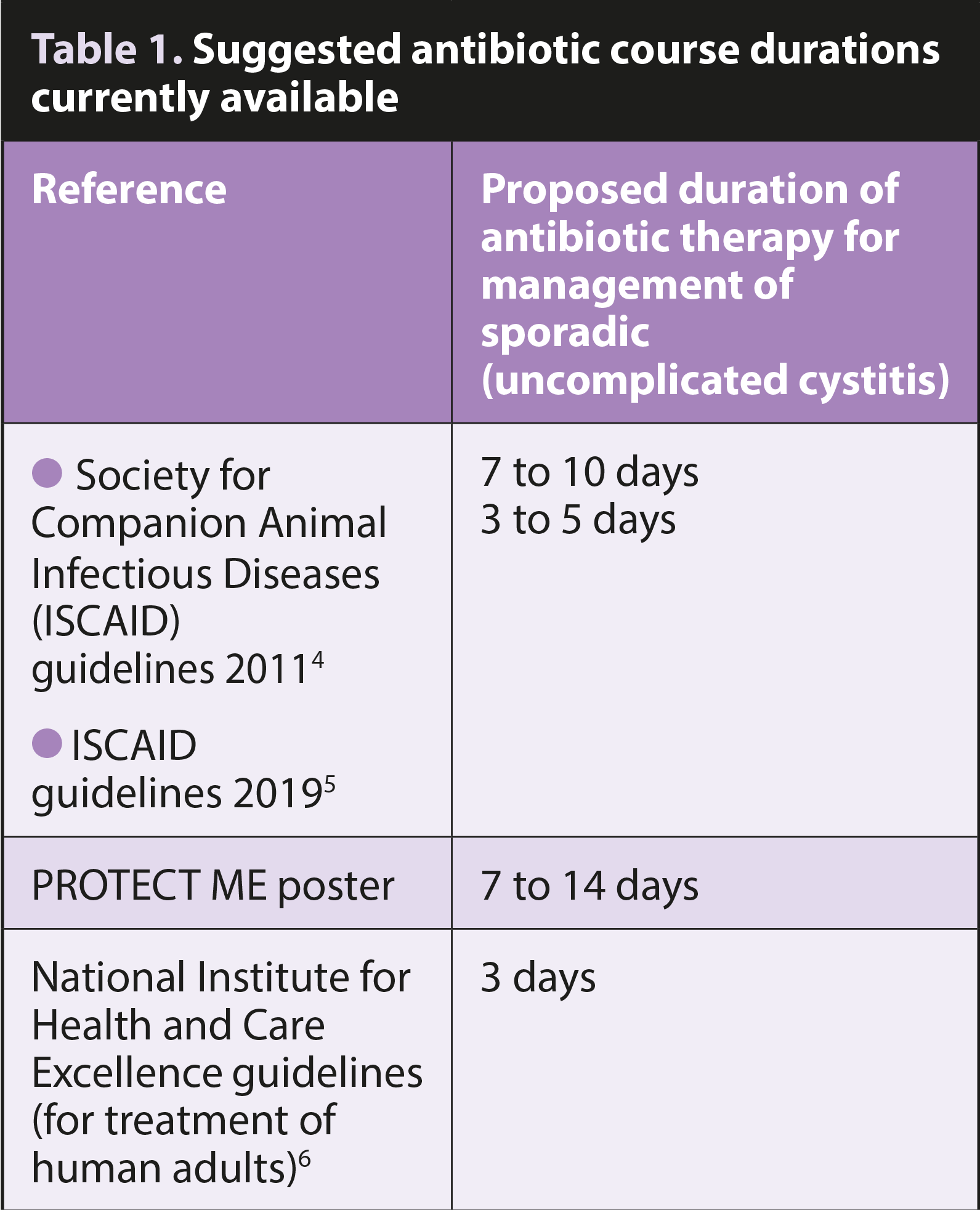
Readers may be aware of the “PROTECT ME” poster produced by BSAVA and the Small Animal Medicine Society, the various International Society for Companion Animal Infectious Diseases (ISCAID) guidelines or wider public health campaigns such as Antibiotic Guardian, Keep Antibiotics Working and World Antibiotic Awareness week.
Their consistent message encourages prescribers (and patients) to avoid unnecessary antibiotic use. However, one area where evidence is sorely lacking relates to antibiotic course duration.
How long should any antibiotic treatment last? Should owners always complete the prescribed course? Will treatment efficacy be compromised by stopping treatment too early?
Randomised control trials have been performed to compare short and long antibiotic courses in various infectious diseases seen in people. This work has been neatly summarised by infectious disease specialist Brad Spellberg in his “shorter is better” table and article1.
The evidence consistently demonstrates non-inferiority (clinical equivalence) of shorter antibiotic courses for conditions including pneumonia, pyelonephritis, cellulitis and osteomyelitis. Such findings enable doctors to confidently prescribe shorter antibiotic courses, thereby decreasing their overall antibiotic use.
Can vets acquire similar evidence to improve their antibiotic stewardship, too?
Two veterinary studies have compared the efficacy of short versus long duration antibiotic courses (of different antibiotics) to treat uncomplicated UTIs. Clare et al compared a 3-day course of trimethoprim-sulfamethoxazole with 10 days of cephalexin2; Westropp et al compared 3 days of enrofloxacin against 14 days of amoxicillin-clavulanic acid3.
In both studies, the shorter course of antibiotics was not inferior in terms of bacterial cure. However, the use of different antibiotics in these studies may not be a fair comparison, and shorter treatment courses may only be appropriate if using select antibiotics.
The optimal duration of antibiotic therapy for management of a UTI in dogs is currently unknown. Table 1 lists some suggested course durations. The evidence base for these recommendations is disappointingly sparse.
A recent study in Canada7 found veterinarians prescribed a median 12 days of antibiotic treatment to manage canine UTIs (consistent with the prevailing guideline recommendations).
While some encouraging signs were seen of a reduction in course length between 2016 and 2018, a risk exists that administering antibiotics beyond what is absolutely necessary could promote the development of antibiotic resistance at remote sites (such as the microbiome).
Hopefully, with increased awareness of the latest guidance, shorter treatment courses will become the norm and total antibiotic consumption will fall significantly.
What is really needed is concrete evidence to support these latest guidelines and reassure prescribers their patients are not at risk of clinical deterioration if given fewer antibiotics.
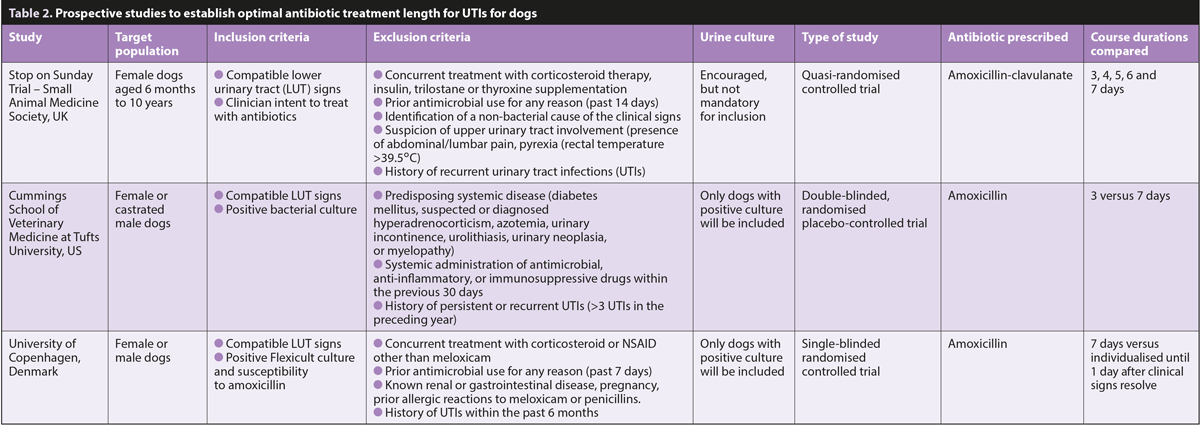
Three different and independent groups have set out to try to generate some data. Teams in Denmark, the US and UK have each designed prospective studies that will help establish the optimal antibiotic treatment length for UTIs in dogs. Each study has its own specific inclusion criteria and will tackle the problem differently. All will rely on the engagement and participation of vets in practice to help generate the vital data. The main features of these three studies are summarised in Table 2.
The presentation of lower urinary tract (LUT) signs (for example, cystitis), is a common reason for consultation in small animal practice accounting for 6% to 12% of antimicrobial prescriptions in dogs.
Antibiotic treatment may be (and likely often is) initiated based on clinical suspicion (a syndromic diagnosis). This may be necessary if it is not possible to aseptically collect a urine sample from a patient or if the owner cannot afford additional diagnostics.
In an ideal world, all antibiotic therapy would be guided by bacterial culture and antimicrobial susceptibility testing. Nevertheless, dogs that present with any of the classic triad of LUT signs (pollakiuria, dysuria or haematuria) have a better-than-average chance of having a UTI8 and this likelihood is even higher in predisposed animals (adult females).
The Stop on Sunday (SOS) UTI study does not mandate the submission of urinary cultures, as the study hopes to mirror, as accurately as possible, the current approach to clinical practice in the UK. This does mean that some non-UTI cases may be inadvertently included in the dataset. The enrolment of any dog to SOS is based on the intention of the participating vet to prescribe antibiotics.
A key principle of antibiotic stewardship is to employ narrow spectrum antibiotics in preference to broad spectrum alternatives whenever possible.
Amoxicillin is effective against Gram-positive and Gram-negative bacteria that commonly cause UTIs in dogs, and is concentrated in urine, allowing it to be effective against some beta-lactamase producing bacteria, too.
In recent guidance produced by the European Medicines Agency’s Antimicrobial Advice Ad Hoc Expert Group, amoxicillin-clavulanate has been placed in the higher category C (caution), while the aminopenicillins (for example, amoxicillin) are category D (prudence). Furthermore, the ISCAID guidelines recommend use of amoxicillin as a first-line approach. This is the antibiotic chosen for both the Danish and American studies.
However, amoxicillin-clavulanate is the most available and most commonly prescribed antimicrobial tablet in Europe, and was prescribed in 44% of all instances of antibiotic use in practices in the UK9.
Due to this widespread availability and commonality of use, amoxicillin-clavulanate was selected for treatment in the SOS study.
The SOS project aims to provide evidence to help in decision making by comparing different treatment durations (three, four, five, six, and seven-day courses) of the same antibiotic (amoxicillin-clavulanate).
Female dogs presenting with a presumptive diagnosis of UTI, based on the presence of dysuria, haematuria or pollakiuria, will be allocated to a treatment group based on the day of presentation.
The name for this study, (Stop on Sunday; SOS), highlights the method of assignment of different treatment durations.
All antibiotic courses will be prescribed such that they finish on the Sunday evening after presentation. For example, dogs presenting on Monday will receive a seven-day antimicrobial course, while those presenting on Tuesday will receive six days’ worth, and so forth. Owners should contact their vet on the Monday (just after completing the antibiotic course) to update the participating vet. They can then reassess the case, and pursue appropriate diagnostic or therapeutic steps, depending on how well the patient is doing. This method of randomisation was selected to ensure effective safety-netting.
Clinical information will be inputted by vets into a data capture system called Castor. This platform will also automatically email owners to collect follow-up data to detect later recurrence.
For the study to provide robust and meaningful evidence, we require a very large numbers of cases (sample size calculations indicate more than 900 cases), so we are asking for interested vets to help recruit cases that they see in practice.
If you are working in veterinary practice in the UK and would consider being part of this study, email [email protected]
Each participating vet will be provided with a unique login to Castor and supplied with all the necessary documents (client consent forms, a user guide for Castor, and copies of the inclusion and exclusion criteria).
With your help, we hope to be able to contribute some robust evidence to answer this question.
Ethical approval for the study has been obtained from the University of Nottingham and an Animal Test Certificate obtained from the VMD.
The full protocol of the SOS study has been published10 and can be accessed by scanning the pictured QR code (Figures 1 and 2).
SAMSoc is actively supporting clinical research in primary care practice. It is vitally important that these populations of dogs are studied so that treatment recommendations can reflect the real world.
In a recent NHS blueprint, it was highlighted that delivering clinical research is everyone’s business and should not be the preserve of clinical academics and specialist research teams11. Taking part in clinical research counts towards your annual CPD requirement and can be logged on the 1-CPD app.
Additional benefits exist from being part of the SOS community, including tailored online CPD events, as well as opportunities to contribute to other stages of the project (data analysis and manuscript preparation) for all interested parties.
If we extrapolate from current practice in human medicine (and infer carefully from results of previous studies in veterinary medicine), some data already exists supporting the use of shorter antibiotic courses to manage UTIs in dogs. However, it would be much better to generate reliable evidence so that veterinary surgeons can manage these patients effectively with the minimal antibiotic required.
Three international studies are striving to provide these answers.
Could you be part of this exciting research too?
The author would like to thank Tina Møller Sørensen and Claire Fellman for their help in preparing this article. Fingers crossed that all of these studies can recruit sufficient cases to generate some interesting results.