12 Mar 2018
With the starting point an x-ray of a two-year-old shorthaired cat with abdominal effusion and a history if dyspnoea, lethargy and anorexia, Francesco Cian asks: what is the diagnosis?
Francesco Cian
Job Title
Figure 1. An x-ray from a two-year-old domestic short-haired cat with abdominal effusion, and a clinical history of dyspnoea, lethargy and anorexia.
Figure 1 is an x-ray from a two-year-old domestic short-haired cat with abdominal effusion, and a clinical history of dyspnoea, lethargy and anorexia.
A straw-coloured ascitic fluid was obtained by abdominocentesis and submitted for analysis. Laboratory data from the fluid revealed nucleated cell count (NCC) 4,500µL, total protein 66gL, albumin 25gL and globulin 41gL. A high magnification photomicrograph of the abdominal fluid is shown in Figure 2 (Wright-Giemsa 50×).
The fluid characteristics (NCC 1,000µL to 5,000µL, total protein >25gL) are supportive of a protein-rich transudate. The submitted smear is characterised by a granular, lightly basophilic background, with very rare red blood cells and scattered bare nuclei.
A mixed population of nucleated cells are present, mostly segmented neutrophils (red arrow), with a lower percentage of macrophages (black arrow) and rare mesothelial cells (not shown). Macrophages often have foamy, vacuolated cytoplasm and rarely show signs of phagocytosis.
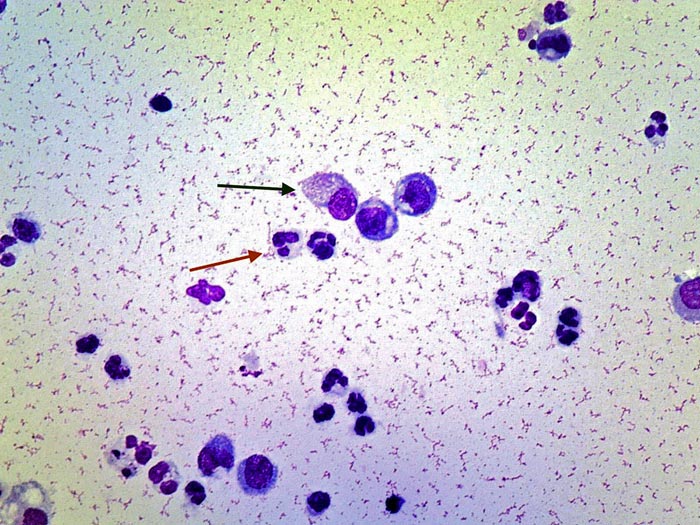
These findings are consistent with protein-rich transudate, compatible with feline infectious peritonitis (FIP) effusion.
FIP is an invariably fatal coronaviral disease causing vasculitis and/or pyogranulomatous lesions in multiple organ systems in a small subset of cats infected by feline coronavirus, undergoing mutation into a virulent form. FIP can affect cats of any age, but is most prevalent among cats less than three years old. FIP has traditionally been divided into two presentations, the effusive (wet) form and non-effusive (dry) form – the former being more common.
The antemortem diagnosis of FIP remains challenging, and it is the combination of signalment, clinical signs and diagnostic aids that will help the clinician obtain a diagnosis. Abdominal distension with ascites, dyspnoea with pleural effusion, jaundice, hyperbilirubinaemia, distinct intra-abdominal masses, uveitis, and a range of neurological signs are all common findings in cats with FIP.
Several direct and indirect diagnostic procedures are available for FIP; however, the sensitivity and the specificity of these indirect tests will vary greatly, depending on the likelihood the cat has FIP (age, clinical signs).
The presence of a characteristic type of fluid in the peritoneal cavity or, less frequently, the pleural cavity, is one of the most diagnostic features of the effusive form of FIP. The fluid is usually yellow-tinged, due to the presence of bilirubin as a product of microhaemorrhage and the breakdown of erythrocytes by macrophages. FIP effusions are classified as protein-rich transudates, as they have variable, low cellularity and high protein content, which explains the granular basophilic background seen on cytology.
A definitive diagnosis for FIP requires identification of viral RNA or proteins within macrophages in characteristic lesions (granulomatous vasculitis) from diseased tissues, and is, therefore, possible only with histological and immunohistochemical examination. Immunocytochemistry of effusions or fluids from cats suspected of having FIP may also be a consideration. However, non-specific positive staining of macrophages may represent a problem in the interpretation of these results.