11 Sept 2017
Sheep lameness is a prevalent issue on UK farms, and, with sheep farming margins already challenging, preventing and tackling it is important, say the authors.

Sheep lameness remains an important sheep flock health issue, with foot rot widespread on almost all UK sheep farms. Lameness is thought to be one of the main reasons for the use of antibiotics on a sheep farm, and it is a condition either requiring the handling of individual sheep, or at least regular gathering.
This adds a cost to the farmer in terms of time and effort, alongside treatment costs and the significant costs of lost production. The gross margins within a sheep enterprise are slim, and having a lameness issue within a flock severely impacts on this.
Lameness is a welfare issue. It is painful and it affects an animal’s ability to graze optimally and function successfully within the flock. It is, therefore, a condition all practitioners should be able to effectively advise on, and positively influence the situation of, on farm.
Sheep lameness is well researched and continues to be studied. This is providing valuable evidence for treatment and control. Within the good practice guidelines, produced by the Sheep Veterinary Society on the responsible use of medicine, is a useful lameness section practitioners may wish to refer to1.

Traditionally, ”scald”, ”strip” or ”interdigital dermatitis” (Figure 1) are terms used to describe inflammation of the interdigital space, often associated with a moist grey/creamy exudate. Once this has progressed to lesions with separation of the hoof from the underlying sensitive tissue with an associated foul-smelling pus, it is referred to as footrot (Figure 2).
Research has disputed the traditionally held assumption Fusobacterium necrophorum was the cause of scald and that further invasion, by Dichelobacter nodosus, subsequently led to footrot2,3.
It has now been shown D nodosus plays the primary role in the initiation and progression of scald/footrot, with an increase in D nodosus load in the week prior to an episode of either scald or footrot, as well as during an episode of scald.
F necrophorum, in contrast, was not particularly associated with scald, but only associated with the lesions once severe footrot was present2,3. Therefore, in adult sheep, treatment plans for both scald and footrot lesions should involve the same protocol.
F necrophorum is a Gram-negative anaerobe found ubiquitously in the soil, environment and in the gut and faeces. D nodosus, a gram-negative anaerobe, was always thought to only survive in soil, off the host, for seven days4, although this has been disputed by latest research suggesting survival on a range of soil types and at a range of temperatures for more than 30 days5.
D nodosus advances into the deeper tissues within the hoof, leading to the development of chronic cases, as well as a reinfection risk to both the individual and the flock. D nodosus has 10 serogroups, with several – of varying pathogenicity – recognised within the UK6.
Simple scald lesions will commonly affect large numbers of weaned or unweaned lambs, associated with wet and moist underfoot conditions caused by poor weather or longer lush or stemmy grass. These cases may be trauma-associated, rather than specifically part of scald/footrot complex, and control strategies can be altered accordingly.
Footrot lesions develop from scald lesions, causing an under-running of the sole and eventual hoof wall separation. The severity of the lesion depends on the strains of D nodosus present, but the foul-rotting odour is detected in all cases. D nodosus macerates and necrotises the superficial and deeper layers of the skin from the interdigital junction with the sole, and extends across to the white line.
Disruption of the capillaries and blood supply of the laminae lead to severe damage and separation, with exposure of the sensitive tissues underneath.
This is a very painful condition and sheep affected with active footrot will appear lame. Sheep with footrot are very infectious to other sheep or lambs at foot, and prompt treatment is essential in its control.
Flocks can be affected by different strains of D nodosus, and the subsequent severity of lameness may vary. They can acquire a level of immunity and resistance to re-infection, although, on the whole, this is short-lived6 and will not offer any significant protection in a flock where the challenge remains high.
However, some individuals are genetically resilient to the challenge of D nodosus infection6 and retaining and rebreeding from these individuals can have huge benefits for the future of the flock.
Contagious ovine digital dermatitis (CODD) is another common infectious cause of lameness, the levels of which are increasing across UK flocks (Figure 3). A farmer survey reported clinical signs associated with CODD were recorded on 35% of 511 randomly selected farms7.
The causative agents have been identified as Treponema species, spirochaetal bacteria with three phylogroups thought to be involved in clinical disease alongside both D nodosus and F necrophorum8.
Clinical differences are seen between CODD and the other infectious causes of lameness. CODD lesions start at the coronary band at the hair-horn junction and start as an area of hair loss developing into an inflamed bleeding ulcerative lesion.
The lesion advances from the coronary band, causing extensive damage to the underlying tissue, and advances towards the sole, causing hoof wall separation and exposure of the extremely sensitive tissues underneath9.
In advanced stages, the entire hoof capsule detaches, exposing the bleeding sensitive tissues underneath. Radiographic studies have revealed significant damage to the bony structures of the foot, leading to osteophytic changes.
Healing lesions have a drier appearance and eventually the hoof wall regrows in a disorganised, less structured way.
Treponema species associated with lame sheep have been shown to be robust and able to survive on hoof-trimmers10 or gloves11 for up to three days following the handling of CODD-infected sheep. In many cases of lameness on farm, multiple lesion types and pathogens present, with treponemes detectable via PCR, as well as both D nodosus and F necrophorum.
It is essential to consider correct diagnosis and not helpful to rely on farmer-diagnosed lesions, as while approximately 80% of farmers can correctly diagnose scald and footrot, only around 50% will correctly diagnose CODD or shelly hoof from photos12.
The presence of mixed infections and correct lesion identification are essential when determining lameness control plans. The authors believe nothing can substitute a veterinary visit to the farm, involving a clinical examination of a representative number of lame sheep.

The risk factors for lameness need to be addressed at the farm level. Failure to do this will affect the success of the lameness control plan and treatment outcomes. The following risk factors can be identified on many farms:
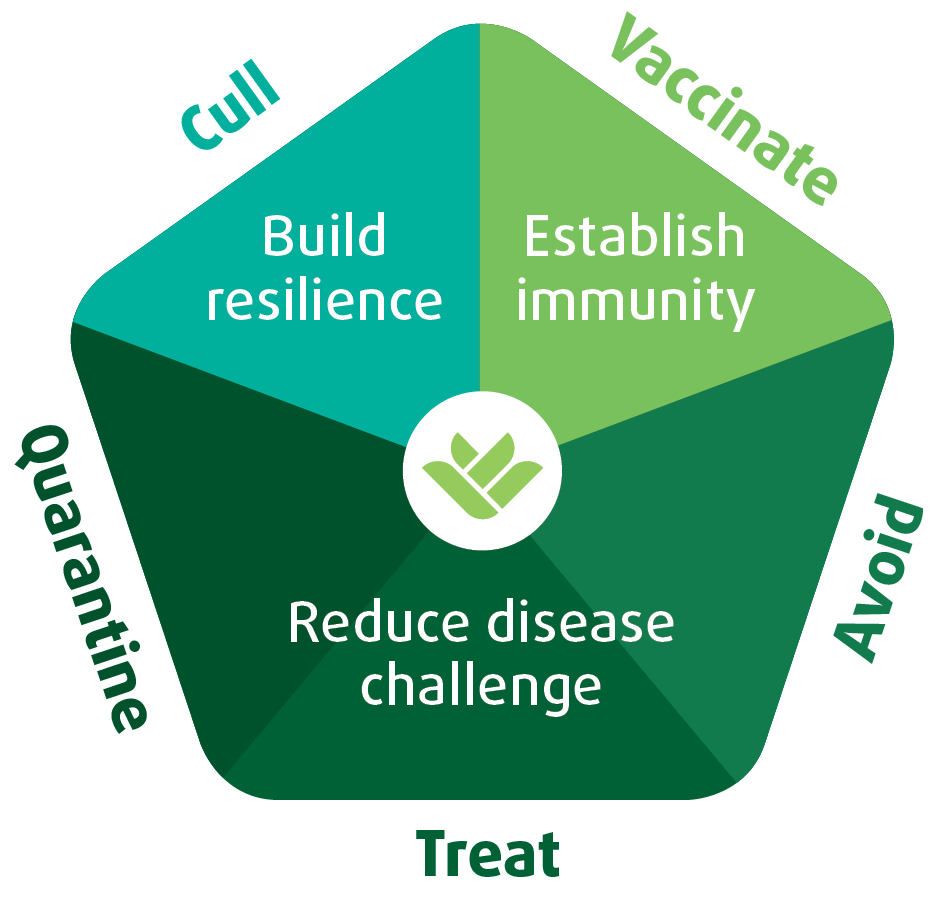
Good evidence is available to support the approach of controlling lameness in sheep. The five-point plan14 (Figure 4) is a well-recognised, industry-led control protocol and it works successfully on farm, providing all areas are discussed between the practitioner and the farmer and application is comprehensive.
The correct treatment, following the correct diagnosis, is a crucial aspect of the five-point plan. The speed of treatment has been well researched and suggests sheep, lame with footrot and treated within three days of becoming lame, have improved treatment outcomes and, importantly, significantly reduce the risk of transmission to other sheep within the flock12.
D nodosus is the primary pathogen in scald/footrot, and so the treatment of adult sheep with either lesion must involve the use of a systemic antibiotic. Treatment of CODD can be problematic due to the level of infection within the deeper tissues of the foot and prolonged antibiotic treatment improves the outcome. The aim for all treatment is to reduce the clinical signs and prevent the development of carrier sheep.
The choice of antibiotic will depend on the on-farm situation, for example, the virulence of the D nodosus serotype, the presence of Treponema species, the presence of suspected resistance, available handling facilities, the location of the sheep and the likelihood of being able to repeat injections if necessary.
Oxytetracyclines are used effectively and offer a prolonged length of action against D nodosus and will still work for CODD on some farms. However, in vitro studies suggest treponemes are most susceptible to gamithromycin and tildipirosin and least susceptible to lincomycin, spectinomycin and oxytetracycline15.
In the field, penicillin and amoxicillin will work to treat both scald/footrot and CODD, but they require injections on a daily or every-other-day basis, depending on the products.
Two newly licensed macrolides are available for treating footrot in sheep: gamithromycin (Zactran; Merial) and tulathromycin (Draxxin; Zoetis). These are useful for their longer duration of action, where repeated injections may not be possible. It is worth pointing out that within the European Medicine Agency-published scientific advice that has been adopted by both the Responsible Use of Medicines in Agriculture Alliance (known as RUMA) and the VMD for the UK, macrolides are not classified as high priority, critically important antibiotics (HP-CIA) in the European context.
Topical application of either oxytetracycline spray or florfenicol spray are a very useful adjuvant to treatment and are useful for both scald and CODD lesions, not least in reducing the spread of infectious agents.
The success of treatment is often judged by an improvement in mobility of the affected sheep. However, often in cases of CODD, where the hoof capsule has detached, the locomotion of the sheep can take an extended time to improve, relating to horn regrowth. This can often be confused with a treatment failure by the farmer, until the hoof is examined.
Once clinical cases surface, the challenge of infection within a flock can be reduced significantly by prompt systemic antibiotic treatment of the infected sheep. The creation of a lame group or ”crock” flock will improve this further by removing lame infected sheep from the main flock and keeping them separate until their lesions have healed.
On a farm situation, it may be impractical to create a crock flock, and prompt treatment of affected cases may not be possible due to labour, handling and time pressures. However, delaying treatment will always delay improvements in the overall lameness levels within the flock.
Lameness is a painful condition and sheep respond well to being treated concurrently with analgesics. Generally, NSAIDs are appropriate and with none licensed for use in sheep, those licensed in cattle can be used under the cascade with the maximum meat withdrawals observed.
Sheep producers are improving in their awareness of the need to treat painful conditions. This can be particularly important in certain times of the production cycle, for example, when ewes need to keep eating in late pregnancy to prevent metabolic disease or when suckling lambs. Sheep producers that have adopted the regular use of analgesia for lameness report significant improvements in recovery.

It may be appropriate to use lime spread in high sheep traffic areas. This raises the pH of the soil and makes conditions less favourable for the survival of bacteria. Anecdotally, farmers report episodes of simple scald in lambs resolving as they are moved into freshly limed fields.
Footbathing is very useful as a disinfectant treatment at handling, quarantine and gathering, provided the handling facilities are suitable. Concrete, hard standing or very dry field conditions are required for footbathing to be useful.
Unless facilities are good, the procedure can be counterproductive and increase the spread of infection, that is, when wet and muddy under foot.
The infectious causes of lameness require prompt treatment with systemic antibiotics to eliminate infection and prevent carrier animals – and, therefore, reducing the overall levels of lameness within the flock. Footbathing alone will not achieve this.
Footbathing can be appropriate for treating groups of lambs with simple scald lesions where it is not thought D nodosus is playing a primary role in disease.
Many footbath solutions are available that include formalin, glutaraldehyde, organic acids, zinc sulphate and copper sulphate. The instructions vary for each solution; some are walk-through preparations, such as formalin, and others require a stand-in time, which is required for adequate penetration.
Provided the instructions are followed, they should all work well for scald lesions in lambs, although note that, whatever the guidance, formalin should never be used at a concentration higher than 3% for sheep.
Considerable pain is associated with the application of formalin to broken skin and severely affected lambs should be separated for topical spray to be applied, rather than them being put through a formalin footbath. If any lifting of the hoof wall is visible, it is appropriate to administer systemic antibiotic, and a number have very short meat withdrawal periods.
Some indications exist formalin will not continue to be available, due to the risks it presents to human health. Understandably, a number of shepherds are choosing not to use the chemical.
The use of antibiotic preparations in footbaths is not authorised by licence and not supported by published evidence of efficacy. Footbaths use high levels of antibiotic, but the lack of clear supporting evidence means these may be administered at sub-therapeutic levels.
This fact, combined with the large potential for inappropriate disposal, presents a considerable risk to the selection of antimicrobial resistance within the environment. For these reasons, the Sheep Veterinary Society Good Practice Guidelines have suggested it is not appropriate to use antibiotic footbaths for sheep.
Control of scald in lambs is controlled on farms successfully using other footbathing preparations. CODD outbreaks require committed treatment plans to improve the situation, with the more severely affected individuals requiring systemic antibiotics. Topical antibiotic sprays are useful, but unrealistic in large flock scenarios.
Zinc sulphate and organic acid preparations (for example, Healthy Hooves) have been used to reduce clinical signs in large outbreaks successfully, and so their use should be considered.
It is well established routine foot trimming in a flock is associated with higher levels of lameness, particularly when a number of sheep are reported as bleeding during this routine trim12.
Research also suggests foot trimming sheep that are lame due to an infectious cause will not improve the treatment outcome and may delay treatment16. Trimming the horn away from an infected foot removes protection of the lesion and may cause further inflammation as trimming advances close to the inflamed lesion.
When explaining this advice to sceptical farmers, the authors generally say: ”Sheep feet may become overgrown when they are infected. They don’t get infected because they are overgrown. It is important to treat the infection, but not necessarily to trim the foot.”
When foot trimming does take place, it should be considered as a cosmetic procedure and great care should be taken to ensure further damage does not occur. The removed horn clippings are infectious, so pose a risk of spread to in-contact sheep. The foot trimming implements become contaminated, so may act as a source of infection to other sheep. This has been demonstrated despite disinfection: treponemes were still isolated on hoof knives following trimming of CODD-infected feet after disinfection10.
Establishing effective control and improving lameness within a flock takes time and significant veterinary input, as well as farmer compliance. It is particularly important new incoming animals or animals returning from ”tack” grazing are considered to be breaches of flock security and treated as sources of infection until proven otherwise.
The only way to reduce this risk is to appropriately quarantine the animals and protect the home flock security. These should include the following measures:
Within a flock, individuals have increased resilience to the lameness-causing infections, particularly any sheep with good hoof conformation and skin integrity.
Heritability to footrot is low to moderate (0.18 in a study of more than 11,000 individual Texels17). Some sheep-breeding strategies incorporate footrot scoring protocols with the aim of generating estimated breeding values (EBV) for footrot.
To date, in a study of resistance to footrot in Texel sheep, no major genome-wise significant quantitative trait loci (QTL) have been identified17.
Flocks consistently breeding from never-lame sheep should increase the genetic resilience within the flock and a few flocks boast of superior lameness resilience. However, this must be accompanied by good flock security, as the low disease challenge in these flocks may mean high numbers of naive sheep that are particularly at risk should an alien virulent strain of D nodosus be introduced.
The current UK recommendation is any sheep lame twice or more should be culled, although this practice is not necessarily supported by an evidence base except via case studies11. Due to the impact a very draconian culling protocol may have on flock economics, the authors generally recommend culling after three episodes of lameness.
Unless the shepherd keeps very good records, this practice is difficult to implement on farm and farmers are always quick to point out it is not possible to cull a lame sheep due to transport rules.
Advice should emphasise every lame sheep should be clearly marked and promptly treated, with records kept.
Ideally, all lame sheep should be separated from the main flock, which should make the identification and record-keeping simpler. Once a sheep is identified as lame for the third time, she should be given her final effective antibiotic treatment and very clearly marked as a cull. As soon as she is sound to travel and the market is favourable, she should be transported off farm as a cull.
If her lameness fails to resolve, she should be euthanised on farm. These ewes will be a constant cost to the farmer due to repeated treatments and infection risk to the flock, and can never provide a financial return.
The footrot vaccine (Footvax; MSD) reduces the clinical signs of foot rot lesions and provides protection against infection with D nodosus serotypes for a period of up to four to five months. It is, therefore, very useful as a treatment to reduce clinical signs and as a preventive procedure.
The inactivated vaccine protects against 10 serotypes of D nodosus, several of which are present in the UK. Infections are often mixed and D nodosus is thought to play a role in CODD infections18, so the use of the footrot vaccine is likely to have a positive role in flocks – even when both D nodosus and Treponeme species are present.
Successful use of the footrot vaccine relies on sound advice and consultation with the veterinary practitioner and individual farm assessment. When used with other control measures, it can significantly reduce the prevalence of lameness within the flock12,18.
The use of the footrot vaccine has demonstrated the largest impact in flocks with high levels of disease12. If used inappropriately, it can be perceived to be expensive and unsuccessful, and so careful consideration and discussion is required.
Lame sheep showing clinical signs should be vaccinated and treated with antibiotic injection at the same time. The remainder of the flock should be vaccinated and it is important the whole flock is vaccinated to reduce the overall on-farm challenge.
Usefully, if any sheep with lesions were missed during those handling periods, they will have received the vaccination, and so levels of overall lameness should reduce.
The level of challenge within the flock can be used to determine the number of vaccinations required. In flocks with high levels of lameness, that is, usually a flock with an established lameness problem, a second vaccination six weeks following the first will be required.
It is recommended the flock should be visited five weeks after the start of a lameness control programme to establish the effect of the vaccine and treatment. If levels are still high, namely greater than 5% of the flock, then a second vaccination should be recommended. One vaccination may be sufficient in flocks where clinical cases have been treated successfully and promptly and where all other aspects of the five point plan have been followed.
The footrot vaccine can be used preventively before the risk periods. This is usually at or after weaning (and shearing), to protect the upcoming tupping period, and during the autumn. It is then recommended again at scanning to protect the housing period or winter period, incorporating lambing and early lactation.
Once lameness control on the farm has been established and a robust control plan is in place, the frequency of vaccination may be reduced to a yearly vaccination at scanning time. Computer modelling of the costs of lameness suggests a cost benefit to vaccination when levels of lameness due to foot rot are greater than 2%19. In some flocks that have achieved low levels of lameness (lower than 2%) and with strict quarantine procedures, or that have become a closed flock, vaccination may not be needed on a regular basis and can be reserved for risk-based use.
It is useful to discuss this aim with farmers to increase compliance with a lameness control programme, and to discuss the aim of an overall reduction in cost of treatment and control.
Effective lameness control relies on the successful application of all of the control measures discussed in this article. Reliance on just one or two methods will not establish successful control.
Many farms rely on footbathing, foot trimming and intermittent treatment strategies, and they consequently still suffer from significant levels of lameness.
When underfoot conditions improve, the apparent effectiveness of these lameness control methods appears to be successful in the short term. However, because the level of challenge and flock immunity has not been addressed, a change in environmental conditions or the introduction of CODD or an alien strain of D nodosus means levels of lameness can increase dramatically within the flock.
Once a successful control plan is in place, it is essential the issues of flock security are fully considered, with a quarantine plan strictly adhered to. All steps in the control plan require specific on-farm discussions between the vet and farmer.
As practitioners, we should be prepared to demonstrate the costs associated with the lameness and be honest about the ”vet and med” costs associated with the initial control plan. Many case studies support the success of developing specific control plans, on close veterinary advice, with an ongoing reduction in the amount of antibiotics used and the labour costs associated with maintaining the reduced levels of lameness.
Tackling a lameness issue is a great opportunity for a keen and knowledgeable sheep vet to demonstrate his or her value on farm, as the discussion and control of lameness should form a major part of the flock health plan.
The advising practitioner should be confident in offering sound, up-to-date advice and be prepared to revisit the flock to monitor progress. This will positively influence the outcomes of advice on the farm, it will strengthen the vet-farmer relationship and it will be clinically satisfying for the vet.