26 Mar 2018
Oliver Tilling discusses how to identify the causes of this common condition and some of the available treatment options.
Oliver Tilling
Job Title
A total of 48.2% of all calves in the UK suffer from scour1 (Figure 1).

It is the most common cause of morbidity and mortality in pre-weaned calves2, accounting for up to 50% of all pre-weaned mortality3. In severe outbreaks, scour can cause 20% mortality of affected calves4. But calf mortality only represents a small proportion of the financial damage an outbreak can cause. Scour costs at least £44 per calf affected, excluding labour5.
In addition, a delay exists in reaching age at first calving and lower yields in first lactation.
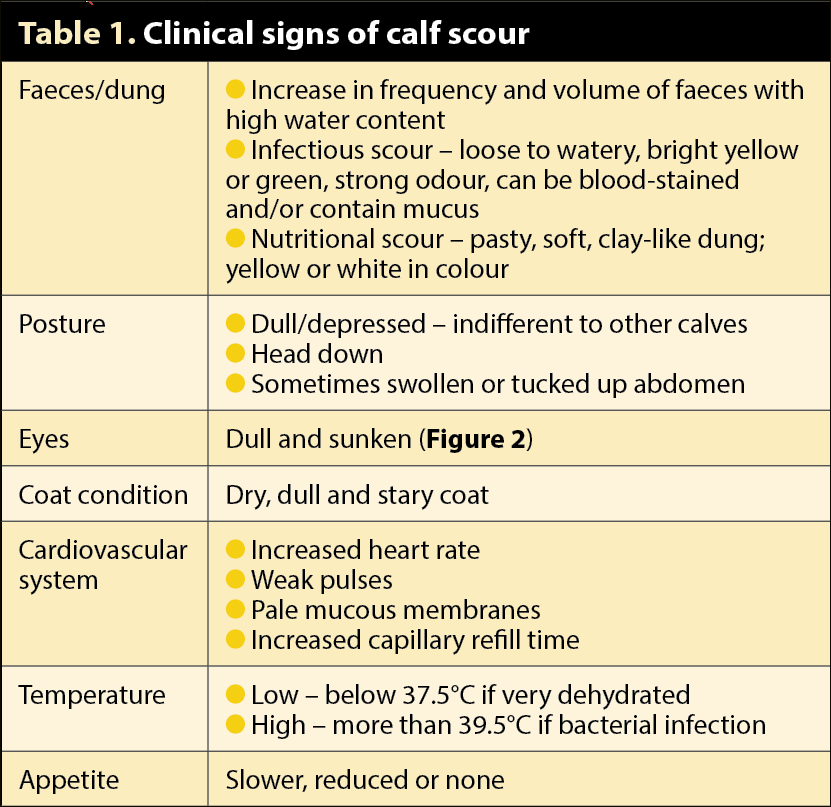
Many infectious and non-infectious causes of scour exist and, as clinical signs are general, it is not possible to identify or predict a specific cause from clinical signs alone (Table 1). The infectious bacteria, viruses and protozoa that cause scour are important, but they can also be found on farms with or without clinical disease. Furthermore, mixed infections with one or more agents are common.
Outbreaks are multifactorial and an interaction between the environment, management, feeding and the pathogens6. An understanding is needed of why an outbreak has occurred, as much as the infectious agents involved.
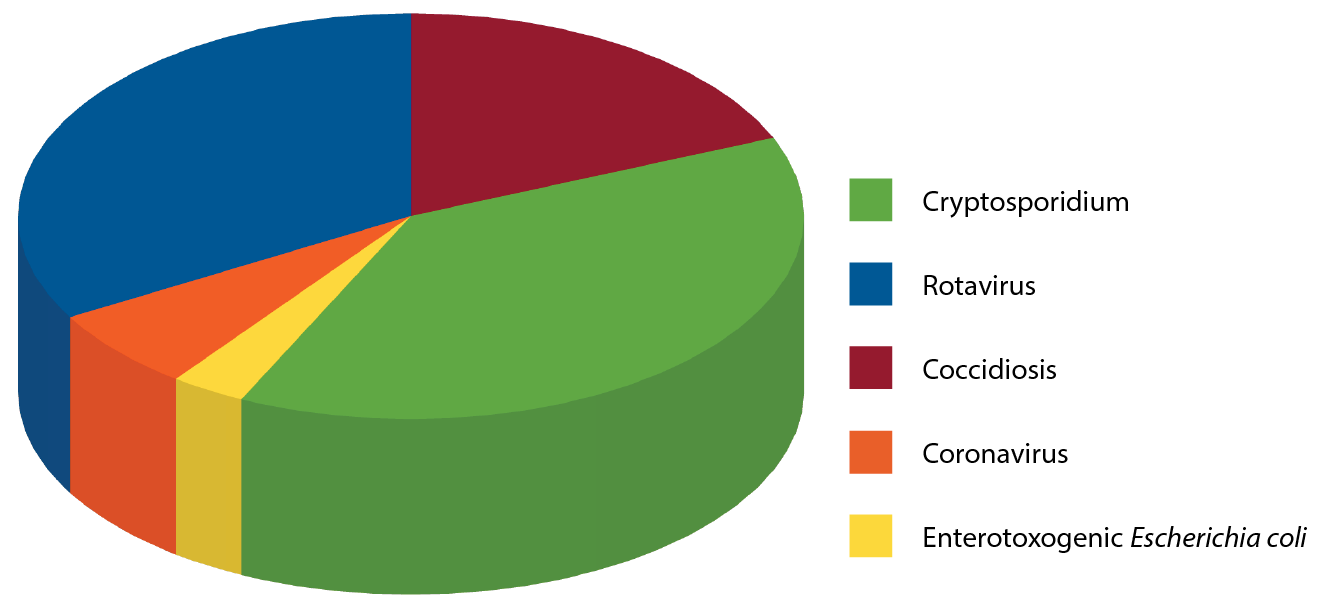
Although many infectious agents have the potential to cause scour in calves, six pathogens are significant:
Figure 3 shows their frequency of diagnosis in the UK between 2006 and 2013.
The most common source of infection is faecal contamination from cows, or other infected calves with scour. These viruses target enterocytes of the small intestine, multiplying and destroying them, so the calf is unable to digest the lactose in milk, and unable to fully absorb water, electrolytes or nutrients.
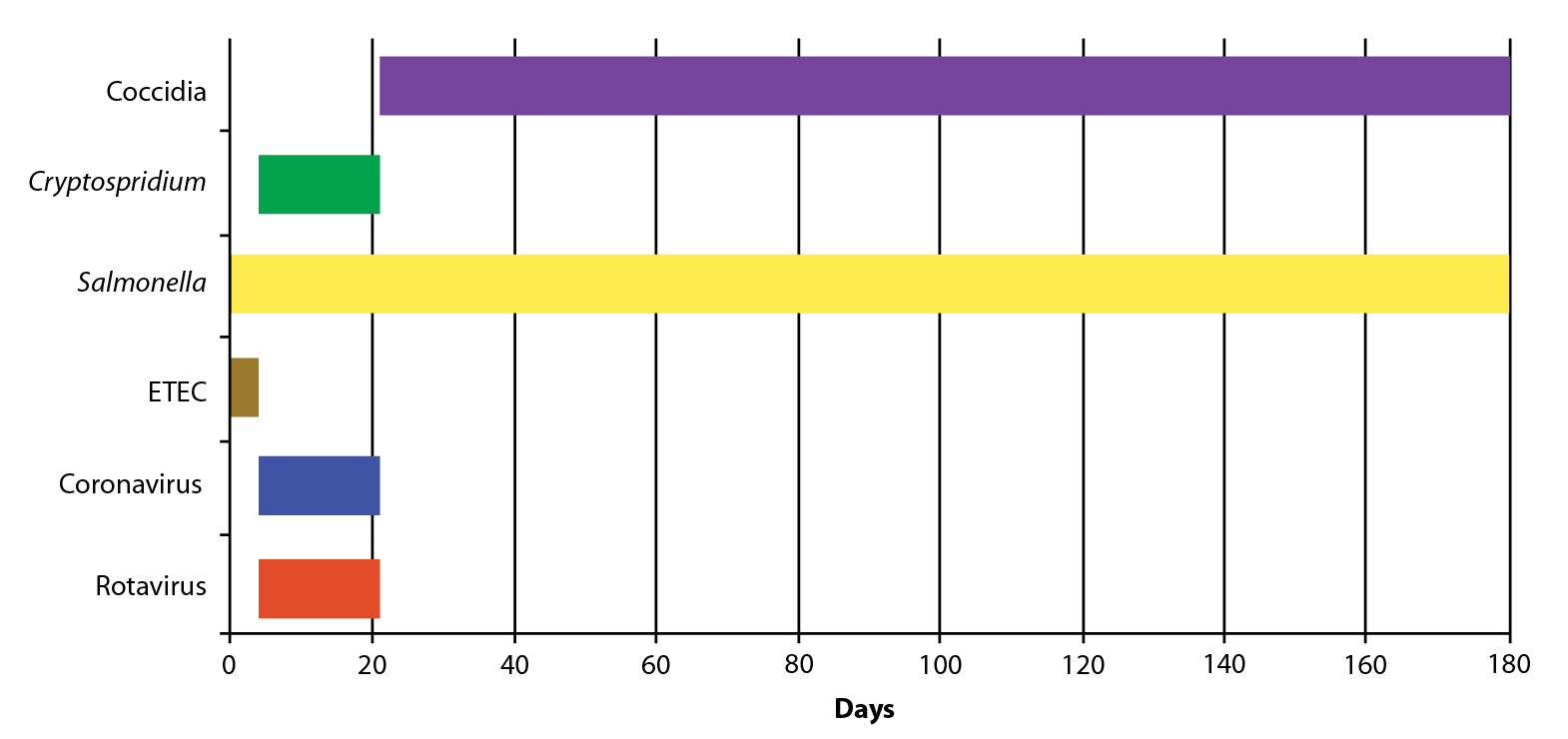
Scour is usually 4 days to 3 weeks of age, with a peak incidence of 6 days for rotavirus, and 7 to 10 days for coronavirus. Older calves can sometimes be affected, too. The ability of the intestine to replace enterocytes is not damaged, though, so gradual replacement with new cells takes several days and the calf will recover after five to seven days8 (Figure 4).
A calf becomes infected with many different strains of E coli within hours of birth. This constantly changing population of organisms inhabits the calves’ intestines for life, which is normal and healthy. However, some strains such as E coli K99 (ETEC), behave differently.
ETEC sticks to the lining of the intestine and produces toxins that reduce normal absorption of sodium and fluids, and stimulates secretion of body fluids into the gut that are then lost in scour8. The high levels of secretion lead to very watery scour and rapid dehydration. This severe scour occurs in the first four days of life and is often fatal.
Many Salmonella species can cause scour, but S dublin is the most common in the UK. Any age of animal can be affected, but disease usually occurs between two and six weeks of age.

Scour is often profuse, watery and fatal (Figure 5). S dublin can also enter the blood stream causing systemic infections, such as pneumonia, septicaemia and joint ill.
This protozoa causes scour in many species, including humans. The source of infection is adult cows. Damage caused is similar to that of rotavirus, with disease occurring from four days to three weeks of age. The infective dose is very low; just five oocysts can result in infection. This low dose contrasts greatly with the parasite’s ability to produce huge numbers of infective oocysts.
Over the 7-day to 10-day duration of a typical infection, infected individuals may shed 10 billion oocysts, with faecal oocyst counts in the order of a million per gram9. The oocysts are resistant to most commercially available disinfectants and can stay alive on the farm for many months, so hygiene is important for control8.
This protozoa causes scour between three weeks and six months of age. Infection can produce chronic scour, or severe haemorrhagic scour with mucus and straining to pass faeces. Only 5% of infected animals show clinical signs of coccidiosis10, with 95% subclinical. Subclinical coccidiosis has the greatest effects on a herd, with ill thrift and poor growth rates. Calves usually recover from scour within 10 days, but some severe cases have a prolonged recovery.
Non-infectious scour – usually referred to as nutritional scour – can occur anytime pre-weaning.


Scour is best considered a failure of intestinal uptake of sodium and water sufficient to overwhelm the compensatory capacity of the colon11. In the healthy calf, a flux of fluid and electrolytes with net secretion occurs proximally and net reabsorption occurs distally, with 90% of net reabsorption occurring in the lower small intestine and the remainder in the colon. The colon operates at only about 40% of its absorptive capacity in the healthy calf, so has considerable functional reserve capacity.
Scour is only seen when this reserve has been overwhelmed such that liquid faeces are produced. Consequently, by the time a calf has scour, the disease process has been in progress for a while11.
Diagnostic testing will influence treatment, prevention and control strategies, which vary for the different infectious causes of scour. A thorough history and observation of feeding management will help determine if a nutritional scour is occurring.
Collection of six faecal samples (minimum 15g each), from untreated calves in the early stages of disease, gives the best possible chance of a diagnosis. Samples must come direct from the rectum and not the floor where they would be contaminated. Samples should be tested for all potential causes of infectious scour – while taking into account the age of animals affected and clinical signs.
If any calves have died then a postmortem examination (Figure 6) is an excellent way to reach a diagnosis – preferably at an approved laboratory where any necessary follow-up testing can be performed. Calves must have died less than 24 hours earlier to give the greatest chance of reaching a diagnosis.

The aim of treatment is to help the calf survive the episode of scour in as good a shape as possible. Treatment must focus on replacement of pathological losses, correcting acidosis, meeting nutritional requirements and, in some instances, the administration of antibiotics12.
Calves with scour lose an average of about 10% (but up to 20%) of their bodyweight in fluid, in addition to normal losses13. For this reason oral rehydration therapy (ORT) is the single most important treatment (Figure 7), and is usually successful if instigated immediately after the scour has developed. ORT is formulated to correct or prevent water and electrolyte deficits, and metabolic acidosis. Oral rehydration solutions should contain13:
Continued feeding of milk is essential for the scouring calf. Milk has natural antimicrobial properties and is highly digestible, so is the ideal nutrient support to the scouring calf14. Continued milk feeding not only provides the energy required for weight gain and growth throughout scouring, but also provides the nutrients necessary for the recovery of the intestinal epithelium13.
The author advises two extra feeds of 2L ORT daily, with milk feeds in between. For example, in a twice-a-day-fed calf: ORT – milk – ORT – milk. Each ORT feed needs to be separated from milk feeding by at least two or three hours; this is due to ORT interfering with the clotting of milk in the abomasum when whole milk or skimmed milk replacer is fed. This can be done for three days, but, if no improvement is seen, further veterinary guidance is recommended. Acetate-based solutions are the best choice for diarrhoeic calves still receiving milk, because acetate does not interfere with abomasal milk clotting14.
A general rule is if a calf is standing it should receive ORT, if it is collapsed (Figure 5), or cannot stand without assistance, it should receive IV fluids. Exceptions are:
It is often necessary to administer IV fluids (IF) on farm, but, preferably, patients should be hospitalised if facilities and biosecurity issues allow. The primary aim of IF therapy is to correct hypovolaemia and, in some circumstances, dehydration. By restoring blood supply to the kidney, it allows many complex acid-base derangements to be corrected rapidly without causing further iatrogenic derangements15.
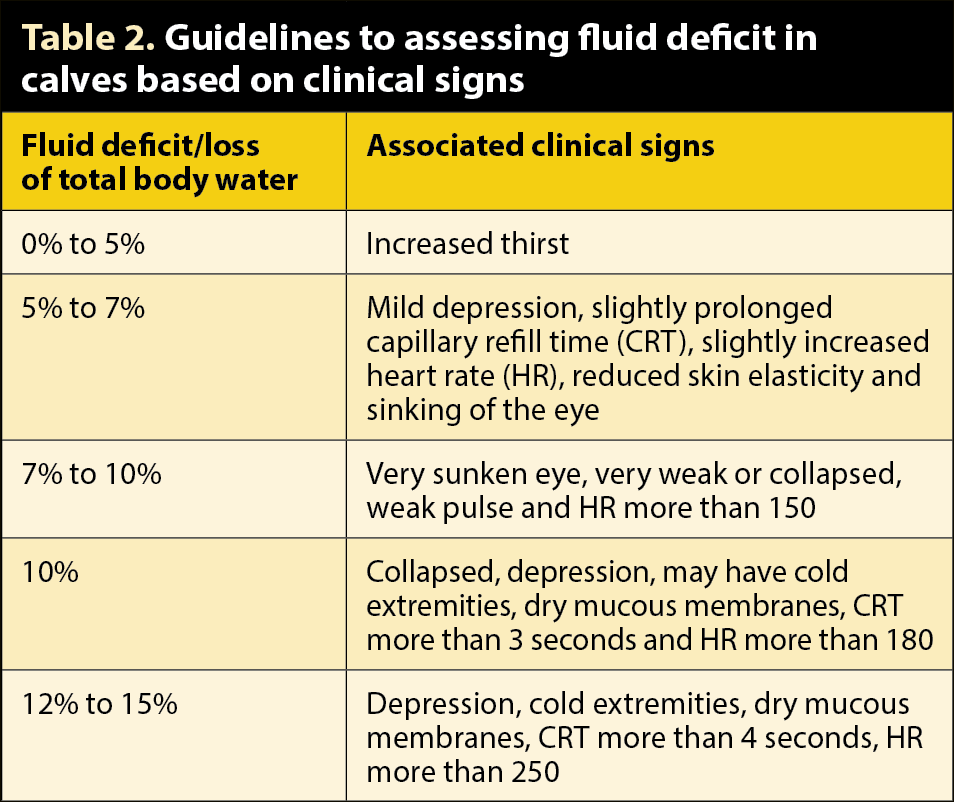
The most practical and useful IF in calves are blood and lactated Ringer’s (Hartmann’s) solution15. Calves have a larger extracellular fluid compartment compared to adults, so their maintenance requirements are double at 5ml/kg/hour or 120ml/kg/day16. The author provides half the fluid deficit as a bolus using Hartmann’s, then the other half of the deficit plus maintenance over the following six hours. Determining the level of fluid deficit is notoriously difficult, but crudely assessed using guidelines in Table 2. Reassessment is made to determine if further IF is required or if fluid administration can be provided orally.
Administration of bicarbonate with IF should be reserved for animals over seven days old that fail to respond to fluid administration or are showing clear signs of acidosis (reduced/absent palpebral reflex and/or severely reduced mentation in the absence of dehydration or other identifiable causes)15. The author uses 250ml hypertonic bicarbonate solution (8.4%) to provide 250mEq bicarbonate and reassess the calf before repeating, if necessary.
The use of antibiotics in calf scour is controversial. The majority of pathogens involved are either viral or protozoal, so do not need antibiotics. However, in calves with scour and severe systemic involvement, intercurrent disease is common and the risk of bacteraemia or septicaemia is increased12 (Panel 1).
Feeding antibiotics to calves to prevent diarrhoea is not recommended. However, calves with diarrhoea and systemic signs of illness should receive injectable antibiotics targeted towards coliform bacteria in the blood (due to likelihood of bacteraemia) and the small intestine (due to bacterial overgrowth). A calf is bacteraemic when exhibiting inappetence, dehydration, lethargy or pyrexia17.
Calf scour causes abdominal discomfort – so analgesia is required. An NSAID will decrease inflammation in the gut and reduce the effects of endotoxaemia and septicaemia. This should encourage feeding and aid recovery, but must only be administered when a dehydrated calf is receiving ORT. If the calf is hypothermic, the use of a heat lamp or calf blanket will help recovery.
Some causes of infectious scour have specific licensed treatments, such as halofuginone for Cryptosporidium. Halofuginone can be used as both a treatment and preventive. It reduces disease severity and oocyst output – minimising further spread. On a group basis, prophylactic use of halofuginone can prevent further scour due to Cryptosporidium after a diagnosis has been made. The drug is given daily for seven days. It has a narrow safety margin and is toxic at twice the therapeutic dose, so ensure the recommended dose is given. Calves with scour for longer than 24 hours should not be treated with halofuginone, and dehydrated calves should not be treated unless on oral fluids.
If Salmonella or ETEC are identified then antibiotics should be prescribed. Antibiotic sensitivity testing will enable appropriate antibiotic selection. If coccidiosis is diagnosed anticoccidial drugs can be used and, if creep feeding calves, then medicated feed is likely to be the most efficacious and simplest method of treatment8.
Irrespective of the causal agent, route of infection for infectious calf scour is the same – ingestion or inhalation of the organism from an environment heavily contaminated by faeces. Hygiene and cleanliness are paramount and, along with good colostrum, are the key to the prevention and control of calf scour.
Good hygiene must start from the moment the calf is born, as many infections are picked up from the calving area. Hygiene and cleanliness must be maintained throughout the calf-rearing period, with specific care taken to clean and disinfect feeding equipment between feeds (Figure 8), and thoroughly clean the environment on regular occasions and between batches of calves (Figure 9). Scour is 1.9 times as likely when calves are reared on wet bedding, and 0.6 times as likely when disinfection occurs between groups6.
General farm disinfectants are usually satisfactory. However, Cryptosporidium oocysts are highly resistant and persist in the environment for long periods of time. Ammonia-based disinfectants will kill them, but produce highly irritant fumes, so can only be used when the building has been destocked. Alternatively, a broad spectrum disinfectant at a three per cent solution is effective8.
Vaccination is available for many infectious scour organisms – specifically vaccines for rotavirus, coronavirus and ETEC – and a vaccine is also available for Salmonella. Both vaccines require vaccination of the cow during the dry period or the heifer as she approaches calving (it is possible to also vaccinate healthy calves three weeks and older for Salmonella). A vaccine is not a substitute for good management and both vaccines rely on good colostrum management to ensure immunoglobulins are passed from cow to calf.
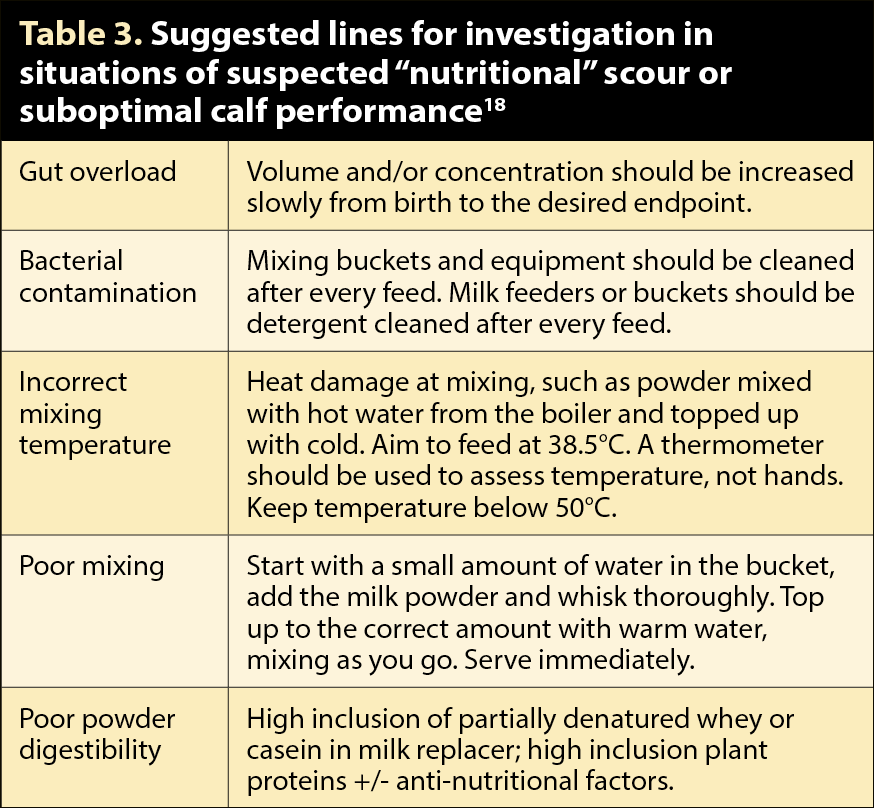
Nutritional scour can be prevented by having a clear, consistent protocol for feed preparation. All feed and equipment must be clean; milk must be mixed at the same concentrations and temperature, and fed in the same volumes at the same times each day. Any changes must be gradual and separated by one week (Table 3).