6 Mar 2017
Moses Brennan highlights factors that can be detrimental to injury repair and provide guidance on strategies to optimise wound healing.
Moses Brennan
Job Title
Assessment is one of the most important steps in wound therapy. More repaired wounds fail because of improper preparation and assessment rather than improper therapy1.

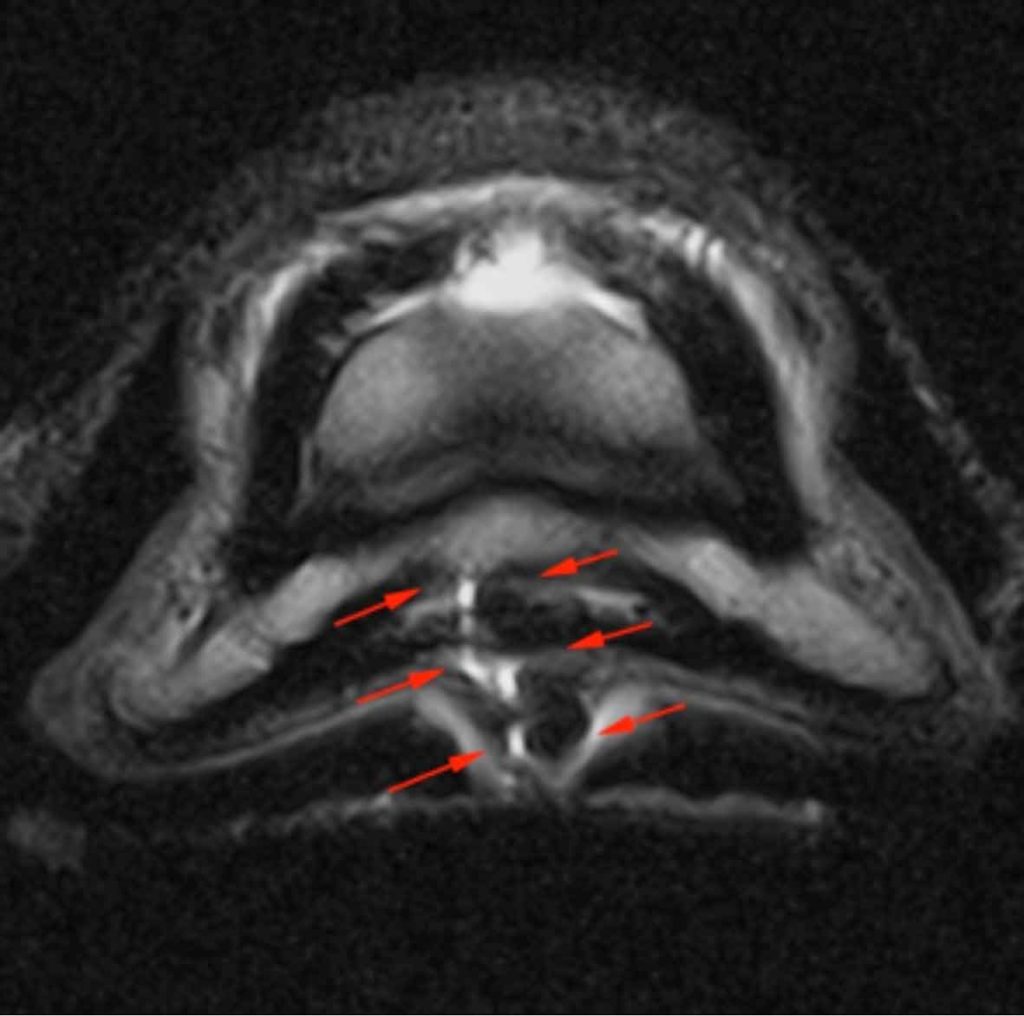
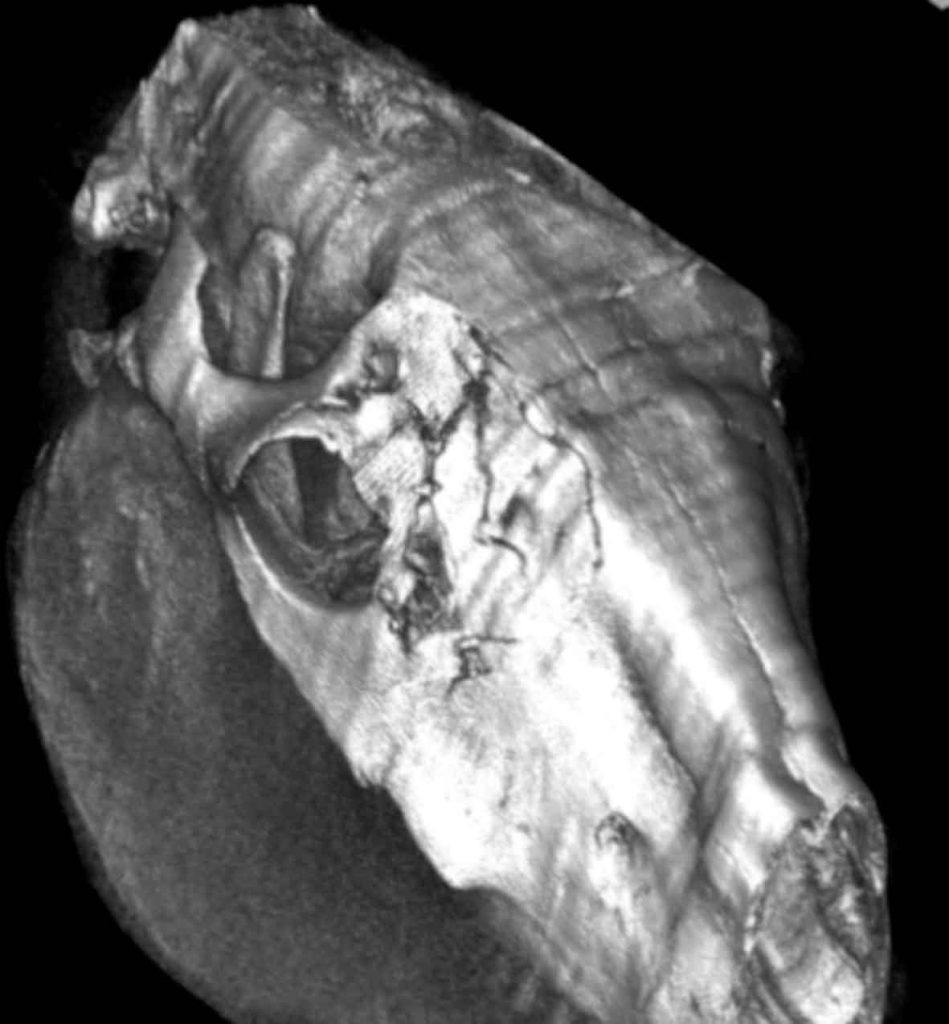
The size and severity of the wound does not correlate well with the true significance of the injury – with small innocuous wounds that result in synovial sepsis often being more difficult and expensive to treat, and potentially having a much worse prognosis for a return to previous athletic function (Figures 1 and 2).
A full assessment of the patient is essential and factors that may delay wound healing should be determined, such as age, vaccination status, physical status, level of nutrition and concurrent systemic disease2.
Assessment and treatment of haemorrhage is important, along with general principles of first aid and stabilisation of any suspected musculoskeletal injury. It is important that, in the field environment, the situation is not made worse by further wound contamination and, after initial triage, it may be more appropriate to move the horse to a clean, dry, well-lit area for further assessment and treatment.
Depending on the nature of the wound, the temperament of the patient and the circumstances, many forms of restraint can be deemed appropriate for initial wound assessment – from simply lifting a limb to full general anaesthesia.

It is often appropriate to use sedation – being aware sedative drugs may result in hypotension and this could result in collapse in a severely hypovolaemic patient. In most instances the use of an α-2 agonist in combination with an opioid will provide adequate sedation. It should be noted, however, in nervous or excited animals – for example, in horses sustaining wounds during strenuous exercise – doses at the “top” of the therapeutic range should be used to achieve a satisfactory level of sedation.
If the wound involves a distal limb then the use of perineural analgesia proximal to the wound location is recommended – this will not only facilitate a thorough examination of the wound, but also facilitates suturing of the wound, if applicable.
Prior to clipping, a water-based soluble gel should be applied directly to the injury to prevent hair sticking to the wound bed. An extensive area of hair around the periphery of a wound should then be removed to allow close inspection of the wound margin and identification of any smaller wounds. Battery-powered clippers are available and can be invaluable when there is no power supply available. After clipping, the periphery of the wound can be cleaned with a topical antiseptic solution, such as povidone iodine or chlorhexidine solution, followed by lavaging the surface of the wound with isotonic saline.
Careful probing of the wound – either with a sterile gloved finger or a sterile probe – should follow to establish the depth and direction of the wound, and ascertain if any deeper structures, such as tendons, ligaments or osseous structures, are involved (Figure 3).
If any suspicion of synovial involvement exists then synoviocentesis of the local structures should be performed. Ideally, a sample should be obtained for cytological analysis (ethylenediamine tetra-acetic acid; EDTA tube) and bacterial culture and sensitivity (plain tube). If it is not possible to obtain a synovial fluid sample then a “wash” of the structure to yield a small amount of fluid for cytology can provide useful information. Additionally, distension of the structure with sterile isotonic fluids and monitoring for fluid egress from the wound will establish if a communication exists with the wound. Leaving the needle in place at the end of sampling and instilling some antimicrobial – for example, gentamicin sulphate – is a sensible precaution against infection, even if the sample appears normal.


When wounds are extensive, obviously extend into deeper tissues, or synovial involvement or significant lameness is apparent, imaging of the surrounding areas is recommended. Radiography and ultrasonography are the two most commonly employed techniques. Radiography will provide information about the osseous structures and ultrasonography is considered useful for soft tissue damage; however, it is also useful to determine the presence of radiolucent foreign material, such as wood or blackthorn, and can also be useful in identifying bony sequestra.
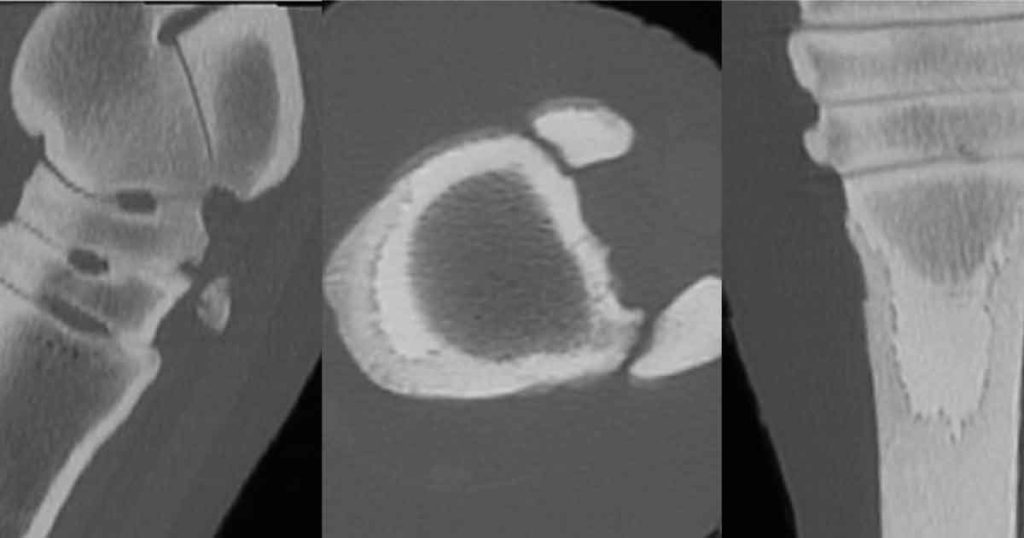
In recent years, a huge increase in more advanced imaging techniques (Figures 4, 5 and 6) has become available and although these techniques are not routinely used, in certain circumstances they can be invaluable in determining the correct treatment strategy and establishing a realistic prognosis for complex cases – preventing treatment that is likely to be unsuccessful. MRI has been widely used to determine which structures are involved in nail penetrations to the solar surface of the foot and is now an established technique to allow accurate treatment of such injuries3.
Equine wounds are frequently contaminated with bacteria, organic debris and necrotic material – making them prone to infection. Early and effective wound debridement reduces the quantity of foreign material present in the wound and greatly reduces the potential for infection to develop. In clean wounds without significant tissue damage, and without significant contamination, effective lavage with a 35ml syringe and a 19G needle4 may provide a sufficient means of wound debridement prior to suturing.
In cases where there is significant contamination or devitalised tissue then surgical sharp debridement with a scalpel provides an effective cost-effective means or vastly reducing bacterial load. In large wounds, such as in Figure 1, sharp debridement can be repeated at regular intervals when it becomes apparent tissue is non-viable.
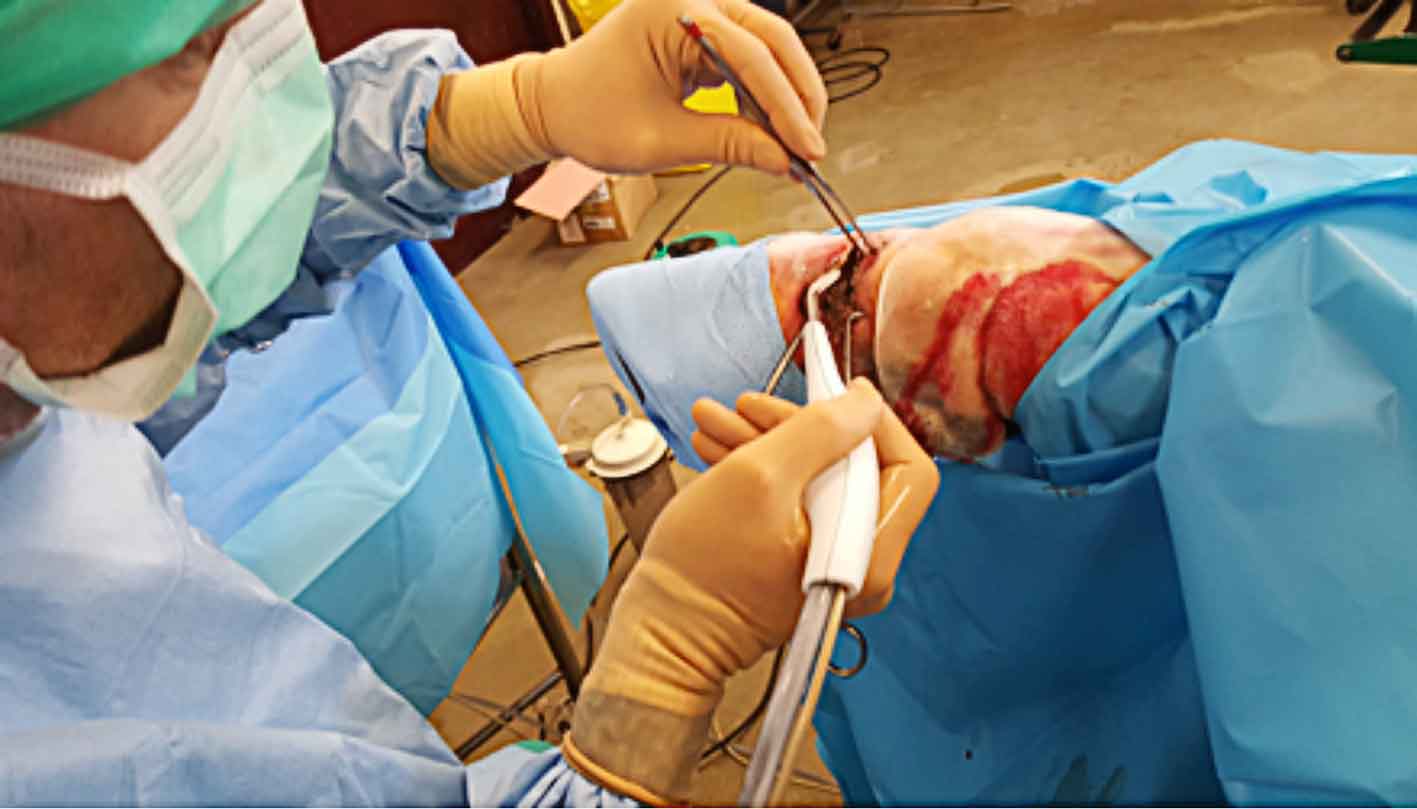
A mechanical hydrosurgery system has been developed that enables a surgeon to precisely select, excise and evacuate non-viable tissue, bacteria and contaminants from wounds, burns and soft tissue injuries5. As the handpiece travels over the soft tissue surface, it creates a smooth wound bed while maximising dermal preservation. The tissue-preserving technique reduces time to closure, which may reduce overall treatment costs5-7 (Figure 7).
The use of wet-to-dry and hypertonic dressings is uncommon and represents a non-selective form of wound debridement, which not only removes necrotic tissue, but can remove desirable epithelial cells and fibroblasts. Autolytic wound debridement, the process of natural wound debridement, is the most selective form of debridement; however, the presence of large amounts of necrotic tissue in a wound bed can potentiate infection and excessive amounts should be removed by mechanical means at regular intervals.
Where possible, and if tissues are viable, wound closure should be attempted unless there is too much tension or tissue loss. The timing for wound closure should be decided on a case-by-case basis and, in some instances, when there is significant swelling, it may be preferable to delay wound closure for a period of one to two days (delayed primary closure). Significant tension is often encountered, especially when closing wounds involving the equine distal limb, and the use of tension-relieving patterns is recommended.
When closing wounds, careful attention should be paid to dead space and drainage of potential wound exudate. Penrose drains provide a simple, cost-effective way to facilitate wound drainage. More complex systems, such as closed suction, can be used in areas that will not drain by gravity. All drains should, ideally, be placed so they do not run directly under the suture line and exit at a site remote to the wound margin. Drains should be removed once the degree of discharge has reduced significantly – in most cases, three to five days is sufficient. Drains left in place for a prolonged period can act as a foreign body and as a source of potential ascending infection.
Wounds that are sutured or wounds to be left to heal by secondary intention need to be covered with an appropriate dressing until primary wound healing or development of a healthy bed of granulation tissue is evident. Many types of primary dressing are available – each having a specific use for each stage of wound healing. It is important to regularly reassess the stage of wound healing and use an appropriate dressing to deal with the wound environment.
The primary dressing should be covered with a bandage with the aim of protecting the wound from further contamination, reduce any swelling by application of even pressure, reduce the degree of motion, absorb wound exudate and provide a moist environment to promote rapid wound healing. The bandage covers the primary wound dressing and is composed of two layers – a secondary and tertiary layer. The secondary layer (for example, cotton wool or Gamgee Tissue) holds the primary dressing in place and provides support to the area, as well as being absorbent if there is significant wound exudate. The tertiary layer secures the bandage in place and provides additional support.
Extreme care should be used when applying bandages to prevent the development of rubs or pressure sores. Particular attention should be placed to the bony prominences of the accessory carpal bone, the medial malleolus of the tibia and the soft tissues of the gastrocnemius and extensor/flexor tendons. If bandages are placed incorrectly, or are poorly managed, the resulting injuries can be worse than the original injury, which is extremely frustrating to owners.
Some locations prone to large amounts of motion will often heal more rapidly by application of a fibreglass cast to provide a more rigid means of immobilisation. Examples include heel bulb lacerations and carpal/tarsal wounds (Figure 8). Although casts are more expensive than bandages, the overall cost can be smaller due to quicker healing times.
A large retrospective study on equine wounds showed primary intention healing was only successful in 24% of horses and 39% of ponies8, indicating most wounds heal by secondary intention. The aim of secondary intention healing is to allow a healthy bed of granulation tissue to develop, without excessive (proud flesh) formation and allow gradual contraction and epithelisation of the defect. In the distal limb of horses, wound contraction is negligible due to a reduced production of TGF-β9 compared with ponies. Wounds that heal by epithelisation are less cosmetic than wounds that heal primarily by wound contraction as epithelial scars or devoid of adnexa10.

Excessive granulation tissue formation is common and reduces the rate of epithelisation of the defect, so strategies to reduce excessive formation should be employed. The most cost-effective method of removing proud flesh is simple surgical removal. The excessive proud flesh should be carefully removed with a scalpel approximately 4mm to 5mm below the skin edge – this needs to be repeated regularly. Topical treatment with corticosteroids can be beneficial; however, short-term use in the early phases of proud flesh formation is recommended. Corticosteroids reduce fibroblast proliferation and the overall inflammatory response; however, they can also have a negative effect on angiogenesis and subsequent wound contraction11.
Vulketan gel (Elanco) contains a serotonin receptor antagonist and has been shown to reduce the development of excessive granulation tissue12.
The use of pinch/punch grafts can be a useful way of promoting more rapid healing in large defects healing by secondary intention, as the grafts exert a significant effect of the development of granulation tissue. The procedure is straightforward and often performed under standing sedation and local anaesthesia.
Several experimental studies have shown the use of bandages can favour fibroplasia and, therefore, be a stimulus to the development of excessive granulation tissue13.
It is important, however, to recognise in the clinical situation, when wounds are extensive, bandaging is often mandatory to prevent further contamination and desiccation of the wound. It is important to remember wounds constantly change, so regular assessment of the healing stage and treatment, and the formation of any excessive granulation tissue, is paramount to achieving a successful outcome.