22 Feb 2016
David Rendle and Moses Brennan outline important factors in the initial assessment and management of ocular injuries in horses.

Figure 12d. Hyphaema and corneal oedema following blunt trauma [a, b]. Tenecteplase was injected [c], resulting in rapid clearance of blood from the anterior chamber [d].
Horses have large globes within prominent orbits that leave ocular and periocular structures susceptible to trauma. They are also flight animals and, by virtue of their temperament, can be highly adept at self-trauma.

Transportation, competition and other activities can further increase the risk of injury. The same temperament that makes some horses susceptible to injury can also render them difficult to treat and the assessment and management of equine ocular trauma cases can be daunting (Figure 1).
The orbital rim comprises the frontal, lacrimal, zygomatic and temporal bones. The frontal bone forms the dorsal orbital rim, while the frontal process of the zygomatic bone and the zygomatic processes of the temporal and frontal bones form the zygomatic arch.
Being the most exposed areas of bone, the frontal bone and zygomatic arch are the most prone to injury (Figure 2). However, the internal orbital wall – made up of the frontal, lacrimal, sphenoid and palatine bones – may also be damaged by forces transferred down from the poll in horses, which sustain trauma to the top of the head when falling.
The ventral orbit, which comprises the lacrimal and zygomatic bones, is rarely damaged. Radiographic assessment is useful in assessing suspected orbital fractures, but CT is the gold standard as it enables better visualisation of the frontal bone and zygomatic arch and enables evaluation of the medial orbit and associated bones of the skull, which cannot be assessed reliably using radiography alone (Figure 3). If CT is not available, lateral, dorsoventral oblique and ventrodorsal (with the plate positioned across the horse’s head) radiographic views should be performed.
Careful comparison of both sides of the face should be performed to identify any asymmetry. Crepitus suggests a fracture is present, while emphysema should prompt investigation of fracture extension into the sinuses. Fractures of the frontal or zygomatic bones can extend axially or rostrally to involve the frontal or caudal maxillary sinus respectively.
Although rare, trauma to the ventral orbit can involve the nasolacrimal duct, and flushing of the nasolacrimal duct and/or dacryocystorhinography may be indicated.



The need for surgical repair of orbital fractures is determined based on the degree of displacement of fracture fragments, presence of fragments that impinge on the globe (or other peri-ocular structures) and the importance of a good cosmetic outcome.
Small fracture fragments are best removed. More extensive fractures of the orbit may be repaired closed or open (DeBowes et al, 1996). The closed technique is more suitable for minimally displaced simple fractures of the dorsal orbit.


More complex fractures, open fractures, fractures more than a few days old and fractures involving other regions of the orbit (the lacrimal bone, zygomatic process of the frontal or temporal bone and zygomatic bone) are better managed by open reduction (DeBowes et al, 1996). Implants may not be necessary if the fracture fragments interdigitate effectively and are self-supporting, but if further stability is required, steel wire, polydioxanone suture or even plates can be used (Figure 4).
Sudden-onset blindness following head trauma and optic nerve damage has been reported in horses (Blogg and Marc, 1990; Martin et al, 1986). Within days of sustaining head trauma, affected horses appear blind and have bilateral, widely dilated pupils. Initially, the fundus and optic discs appear normal, but within three to four weeks pallor of the optic disc, attenuation of the retinal vessels and peripapillary pigment disruption develop.
Eyelid lacerations are common in horses and can occur in isolation or in conjunction with injury to the globe. The upper lid is the more commonly damaged (Figure 5) and is also the more important, as it plays a greater role in distributing tear film and preventing exposure keratitis.
Surgical repair should be undertaken promptly before oedema and inflammation distorts the affected tissue and hampers effective repair – and before (further) corneal damage occurs (Figure 6). The eyelids are amenable to regional analgesia, enabling virtually all repairs to be performed standing under sedation.
Sensory and motor blockade to the upper lid are achieved by supraorbital and palpebral nerve blocks respectively. The supraorbital nerve block only desensitises the centre of the upper eyelid – the lacrimal nerve provides sensory innervation to the lateral portion and the infratrochlear nerve is sensory to the medial canthus. These nerves can be desensitised by infiltrating local anaesthetic laterally or medially along the rim of the orbit. The lower lid is desensitised by infiltrating local anaesthetic along the ventral rim of the orbit to block the zygomatic nerve.
Precise apposition of the eyelid margin is essential if future keratitis is to be prevented. The eyelids are highly vascular and tissue that appears devitalised will often survive (Figure 7). Debridement at the eyelid margin should be avoided if at all possible, as this will distort the normal eyelid margin.



A two-layer closure is typically preferred with a third subcutaneous layer being an option if there is marked oedema. The eyelid margin is aligned first, often with a figure-of-eight, mattress or cruciate suture, which may be preplaced while the first (deep) layer of sutures is placed in the remainder of the laceration. Absorbable sutures (5-0 or 6-0) are placed in the tarsal plate, ensuring the suture material does not penetrate the conjunctiva. The skin can be closed with continuous or interrupted, absorbable or non-absorbable sutures.
With prompt and accurate repair, eyelids have a tremendous capacity to heal and good outcomes can be achieved, even if tears are large or the lids are virtually avulsed. Temporary tarsorrhaphy may be beneficial to reduce the risk of corneal damage while eyelid lacerations heal and normal function returns.
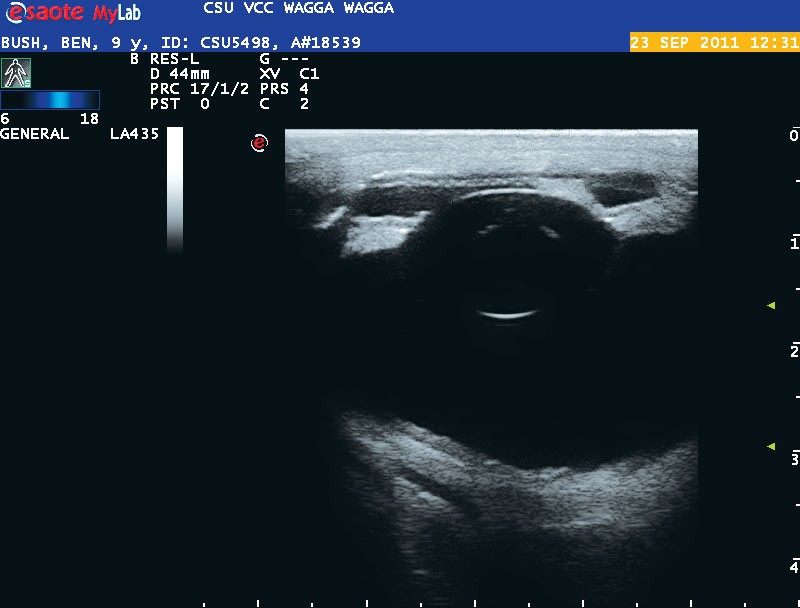
The normal equine globe is virtually spherical, but is slightly flattened in an anterior-posterior plane. In adult horses the globe measures around 48mm high or wide and 44mm deep. In the context of trauma, the best reference for determining whether there has been any change in the size of the globe is obviously the other eye.



Ultrasonographic examination is helpful, but should be performed carefully for fear of opening or worsening a laceration. The anterior chamber is likely to appear more shallow than the contralateral eye (Figure 10) and the pupil may be distorted toward the defect.
When the globe sustains blunt trauma, rupture is most likely to occur at or near the limbus. If the sclera ruptures, the site may be concealed beneath the conjunctiva. Fortunately, the posterior sclera rarely ruptures. Scleral ruptures may occur at more than one site and it may be necessary to perform a peritomy around the rupture site to ensure further tears are not present.


Dilution of the fluorescein stain by egress of fluid from the anterior chamber (with gentle pressure possibly applied to the globe) will result in streaks of fluorescein turning green or dispersing. This test is highly fallible, however, as penetrations are often plugged effectively by a combination of iridial tissue, blood clot and fibrin, and may only leak intermittently or not at all.
Intraocular pressure may be assessed if a tonometer is available, although the same limitations apply and normal intraocular pressure does not eliminate the possibility of globe rupture.
The normal equine cornea varies in thickness from approximately 0.6mm in the centre to 1.0mm at the periphery.
Superficial abrasions to the cornea will generally heal very well and surprisingly quickly. Surgical intervention is indicated if deep laceration occurs and the structural integrity of the cornea is compromised. If the laceration is sharp and clean, suturing it may be all that is required.
With blunt trauma and rupture, the edges are typically irregular and pose a greater challenge. Corneal lacerations are often plugged by uveal tissue and may be left if they are small. However, the result will be an eye with permanent anterior synechiae, a distorted pupil and corneal scarring.
The globe may suffer phthisis over time. Surgical repair is likely to be associated with a better outcome, and larger lacerations that are not repaired surgically will invariably result in chronically painful, and ultimately phthisical, globes. In one report of 15 horses treated for corneal laceration and iris prolapse, the globe was saved in 80% of cases, although not all remained visual (Chmielewski et al, 1997). Resection of uveal tissue did not affect outcome adversely.
Surgical repair of full thickness corneal laceration with iris prolapse requires general anaesthesia and specialist ophthalmic equipment. Surgery involves the removal of damaged or devitalised uveal tissue and the repositioning of healthy uveal tissue within the anterior chamber. Cautery is advisable to control haemorrhage from the uveal tract and prevent hyphaema and glaucoma.
The corneal deficit is closed with sutures placed 2mm apart, so as to be watertight at a depth of three-quarters the thickness of the cornea (Schaer, 2007). The anterior chamber may need to be lavaged and/or inflated with polyionic fluids. Sodium hyaluronate may also be used to inflate the anterior chamber.
In the majority of cases of corneal rupture, further support and an extra seal is provided by means of a conjunctival flap. If a flap is performed, more corneal scarring is to be expected, but this is
a minor concern when preservation of the globe is at stake.
A degree of scarring is to be expected, even if no flap is performed. Third eyelid flaps, or tarsorrhaphy, may be used to provide further support for one to two weeks after the repair has been performed.
Topical antimicrobials should be administered while there is evidence of a breach in the corneal epithelium (that is, fluorescein uptake). Virtually all corneal injuries will be accompanied by a degree of uveitis, which will increase ocular discomfort and should be treated aggressively with topical atropine and systemic NSAIDs to prevent discomfort and reduce the risk of synechiae formation.
Topical ointments should be avoided if there has been a breach in the cornea, as the oil base may enter the globe and increase intraocular inflammation. Following corneal laceration, intensive medical therapy will also be required and a subpalpebral lavage system should be placed at surgery to facilitate medication and reduce the risk of further ocular trauma when battling to apply topical medications. Systemic antimicrobials should also be administered if full thickness corneal laceration has occurred.
A syndrome of trauma-induced, non-ulcerative keratitis with accompanying uveitis has been described (Moore et al, 1998). The authors of this report advise against the use of corticosteroids because of their inhibitory effect on corneal repair and vascularisation. Uveitis was effectively controlled with NSAIDs and atropine. Though not used in the report cited, topical ciclosporin might also be beneficial.
Most trauma to the globe will be accompanied by a degree of uveitis, which manifests as miosis, aqueous flare, fibrinous pupillary membranes, synechiae formation and hyphaema.
Aggressive treatment is important to minimise discomfort, reduce the risk of long-term synechiae formation and help prevent permanent distortion of the uveal tract.
Formation of posterior synechiae is accompanied by a risk of cataract formation, while anterior synechiae disrupt the corneal endothelium and may result in corneal oedema and permanent corneal scarring. The author has used intra-cameral injection of the tissue plasminogen activator tenecteplase to eliminate fibrinous pupillary membranes.
Hyphaema in horses is common in association with trauma (Figure 11). It may resolve spontaneously, once the underlying pathology has been removed (Barnett et al, 2004), and prognosis is reportedly good if blood fills less than half the anterior chamber. However, other authors suggest in the absence of perforation of the globe, hyphaema will usually result in glaucoma and has a poor prognosis (Cutler, 2005).
Further complications of hyphaema include synechiae, cataract formation and phthisis bulbi. Little is published on the treatment of hyphaema in horses, but treatment in humans comprises atropine to minimise synechiae formation and corticosteroids or NSAIDs to decrease intraocular inflammation.
Tissue plasminogen activators, such as tenecteplase, may be a useful adjunct in the treatment of hyphaema and facilitate rapid clearance of blood clot from the anterior chamber (Figure 12; Rendle and Hughes, 2013).
![Figure 12. Hyphaema and corneal oedema following blunt trauma [a, b]. Tenecteplase was injected [c], resulting in rapid clearance of blood from the anterior chamber [d].](https://testing-vettimes-next.sfo3.digitaloceanspaces.com/2016/03/VTE2.1-Rendle-Figure-12a.jpg)
![Figure 12. Hyphaema and corneal oedema following blunt trauma [a, b]. Tenecteplase was injected [c], resulting in rapid clearance of blood from the anterior chamber [d].](https://testing-vettimes-next.sfo3.digitaloceanspaces.com/2016/03/VTE2.1-Rendle-Figure-12b.jpg)
![Figure 12. Hyphaema and corneal oedema following blunt trauma [a, b]. Tenecteplase was injected [c], resulting in rapid clearance of blood from the anterior chamber [d].](https://testing-vettimes-next.sfo3.digitaloceanspaces.com/2016/03/VTE2.1-Rendle-Figure-12c.jpg)
![Figure 12. Hyphaema and corneal oedema following blunt trauma [a, b]. Tenecteplase was injected [c], resulting in rapid clearance of blood from the anterior chamber [d].](https://testing-vettimes-next.sfo3.digitaloceanspaces.com/2016/03/VTE2.1-Rendle-Figure-12d.jpg)


Organic foreign bodies, such as wood splinters, can be difficult to detect if they cannot be visualised directly. On ultrasonographic examination they are likely to cast an acoustic shadow, but if there is extensive tissue damage this may be difficult to identify.
Organic material requires removal that is generally straightforward if it is lodged within the cornea, and, thankfully, it is uncommon for foreign bodies to find their way into the globe. Non-organic foreign bodies, such as splinters of metal or glass, incite less of an inflammatory response, and although they are better removed, they may be tolerated if they are not amenable to surgical excision.
Foreign bodies lodged within the cornea are readily removed with appropriate equipment, sedation and a combination of topical analgesia and regional nerve blocks (Figures 13 and 14). Topical antimicrobials, and possibly antifungals, should be administered following removal of corneal foreign bodies to reduce the risk of stromal abscess formation.
Any injury to the lens is likely to be associated with alterations in lens metabolism and opacity, for instance, cataract formation. Cataracts may be focal or generalised and develop immediately after trauma or weeks later. Luxation or subluxation of the lens will be associated with severely impaired vision and cataract formation.
If the lens capsule is penetrated, the autoimmune response to lens protein will result in a granulomatous endophthalmitis and a poor prognosis for the affected globe. The lens may be removed to preserve the globe or the whole globe can be removed. While removal of the lens will result in a better cosmetic result, enucleation is likely to be associated with fewer complications and less discomfort for the horse.
The prognosis for vision following retinal detachment associated with ocular trauma is grave and enucleation is indicated
(Mätz-Rensing et al, 1996; Rebhun, 2010; Strobel et al, 2007). Retinal detachment is best diagnosed with ultrasound; a characteristic mobile hyperechoic band is evident and usually retains its attachment around the optic disk.
Displacement of the globe from the orbit is uncommon in horses, but when it does occur the prognosis is grave, particularly if the globe becomes trapped in front of the lids.
If the globe is not replaced rapidly, it becomes trapped in front of the swollen eyelids. Arterial blood supply and venous drainage are impaired and the stretching of the optic nerve results in optic neuropathy. Under sedation and local analgesia, the globe should be replaced as quickly as possible.
If the globe cannot be replaced with manual pressure and lubrication, a canthotomy should be performed by cutting 1cm along the lateral canthus (Schaer, 2007). General anaesthesia may be required if this proves unsuccessful. Once the globe is replaced the canthotomy is closed and the globe is maintained in position by performing a tarsorrhaphy with multiple broad sutures and stents. Systemic anti-inflammatories and antimicrobials are indicated.
Trauma may result in herniation of fat through damaged episcleral fascia, which appears as a bulging of the conjunctiva. Treatment requires resection of the fat and closure of the fascial layer and conjunctiva.


Chemosis is common when ocular trauma occurs (Figure 15). The conjunctiva is forgiving and lacerations will repair without suturing. Careful examination should be performed to ensure tears do not involve the sclera, especially when there is subconjunctival haemorrhage.
Peritomy may be indicated if there is chemosis and/or subconjunctival haemorrhage and a globe rupture is suspected, but has not be located.
Prognosis for vision is poor if the retina has detached, the lens has luxated or been penetrated, or if there is severe endophthalmitis. A persistently dilated pupil is likely to indicate permanent optic nerve damage and is a poor prognostic indicator.
The presence of a pupillary light response (PLR) indicates intact retinal and optic nerve function and is an encouraging sign that vision, if apparently absent, may return. The absence of a PLR does not necessarily indicate vision will be lost, but efforts should be made to establish whether the ocular pathology is reversible.
The contralateral eye can be observed for evidence of a consensual PLR if the pupil in the affected eye cannot be assessed. A bright light should be used close to the injured eye to compensate for light attenuation within the injured eye, and to overcome the fact a consensual PLR will always be weaker than the ipsilateral response.
Ultrasonographic examination is invaluable in determining prognosis, especially when pathology within the cornea or anterior chamber prevents visual assessment of deeper structures. The appearance and position of the lens should be determined and the fundus should be examined to ensure the retina remains attached, helping you to determine whether there is sub-retinal haemorrhage.
Corneal lacerations are associated with a poor prognosis for vision if there is penetration and intraocular infection, disruption of intraocular structures, hyphaema above the equator of the globe, a laceration of more than 15mm in length or a laceration that extends through the limbus into the sclera.
If the prognosis for vision is poor, enucleation should be performed to avoid unnecessary pain and suffering. Implants are available for cases where cosmetic appearance is prioritised above a horse’s welfare.