2 Dec 2019
Rachel Agass and Kate Loomes discuss options for long-term analgesia, as well as the use of scoring scales for monitoring the response of patients.

Main image: F.W.P. / Adobe Stock
Part one of this article (VT49.22) reviewed pain pathophysiology and the management of acute pain.
Part two discusses options for longer-term pain management and mentions pain scoring as a means of monitoring response to analgesia.
While systemic analgesia in the short term is often administered IV or IM, oral medications may be relied on for longer courses of treatment.
Common complaints necessitating longer-term analgesia include orthopaedic conditions, such as degenerative joint disease and laminitis.
Importantly, the severity of pain and likelihood of sufficient improvement warrant careful consideration with regards to animal welfare.
Oral formulations of NSAIDs are commonly administered to horses for the medium-term to long-term management of pain. Table 1 lists some of the licensed NSAID preparations.
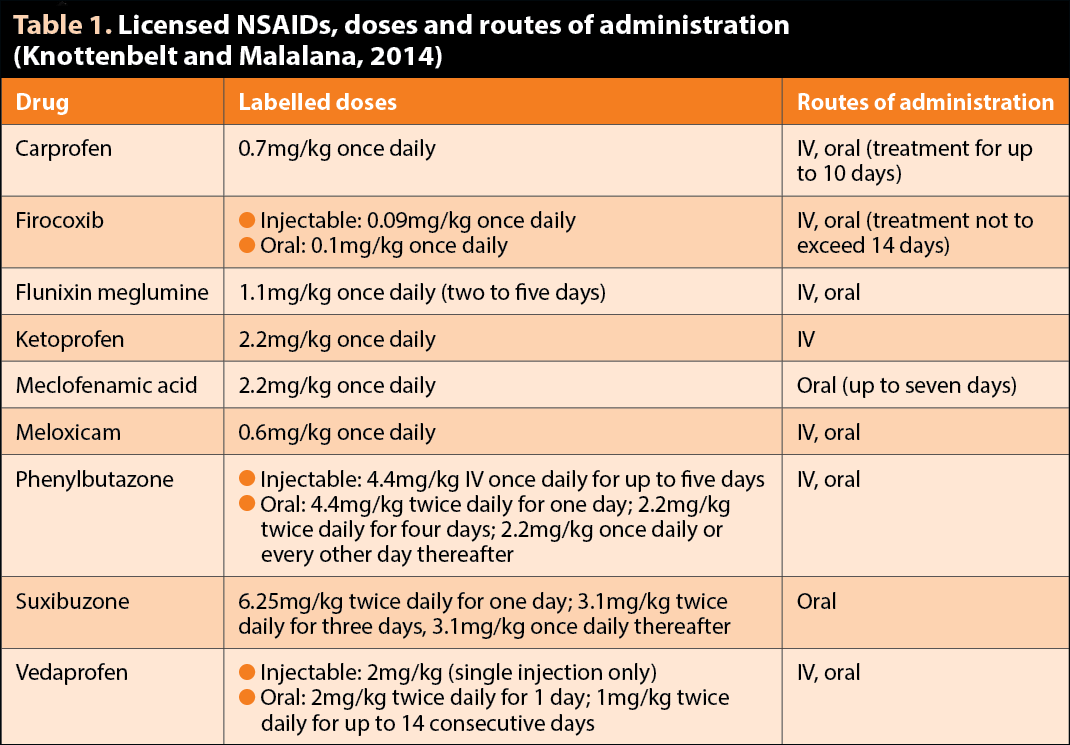
Oral formulations are typically powders, granules and pastes, and are generally well tolerated, although palatability can be an issue.
Concerns regarding toxicity – particularly with respect to longer-term administration – warrant consideration, and these drugs are perhaps wisely used conservatively and reviewed regularly in high-risk patients.
Potential adverse effects of any NSAID use may include gastrointestinal or renal injury, and while experimental work investigating the phenylbutazone safety margin suggests doses that do not exceed 2.2mg/kg twice daily or less are relatively safe (Taylor et al, 1983), the margin of safety is drastically reduced if this dose is exceeded.
Obtaining an accurate weight using conventional methods – such as a weight tape, body score system or scale – is of utmost importance when calculating the amount to be administered (Goodrich and Nixon, 2006).
Acute phenylbutazone toxicity in horses resulting from overdose is characterised by mucosal ulceration throughout the gastrointestinal tract, oral ulceration, renal papillary necrosis, vasculopathy, thrombosis, protein-losing enteropathy and hypoalbuminaemia (Sanchez, 2009).
Horses with large intestinal disease, resulting from NSAID toxicity generally, are receiving inappropriately large doses or have underlying disorders that predispose the large intestine to the toxic effects of NSAIDs, even at appropriate doses (Sanchez, 2009). Ulceration and stricture of the right dorsal colon was seen in four horses after chronic phenylbutazone therapy exceeding recommended doses (Hough et al, 1999).
In normal, hydrated animals, inhibition of the production of prostaglandin I2 and prostaglandin E2 by administration of an NSAID has little effect on renal haemodynamics.
However, in a volume-depleted or dehydrated animal, administration of NSAIDs inhibits locally produced prostanoids that may lead to the characteristic lesion of renal papillary necrosis seen with NSAID toxicity (Read, 1983; Cook and Blikslager, 2015).
A 24-hour period should be allowed to elapse between the administration of two different NSAIDs, since the concurrent use of NSAIDs can have severely detrimental effects. One study demonstrated severe hypoproteinaemia, hypoalbuminaemia and colitis in all horses administered a combination of phenylbutazone (2.2mg/kg orally twice daily) and flunixin meglumine (1.1mg/kg IV twice daily) for five days. Horses treated with phenylbutazone alone did not have significantly different protein or albumin concentrations compared with controls (Reed et al, 2006).
Investigation of the use of cyclooxygenase-2 (COX-2) selective NSAIDs in horses, such as firocoxib, has been performed in an effort to reduce adverse effects associated with decreased prostaglandin production on renal and gastrointestinal blood flow.
A clear benefit to the use of COX-2 selective drugs has not been demonstrated in horses. Therefore, the choice of drug often depends on availability, cost and clinician preference.

Treatment should be discontinued if gastrointestinal side effects occur and serum albumin concentrations should be examined if cause for concern exists.
In healthy adult horses, daily oral administration of meloxicam at 0.6mg/kg was well tolerated for six weeks without drug accumulation in plasma (Noble et al, 2012).
In a large multicentre study, administration of firocoxib paste (0.1mg/kg orally every 24 hours) significantly improved lameness scores, and comfort and mobility in most horses treated because of naturally occurring OA. Adverse effects were infrequent (fewer than one per cent of horses); they were mild and resolved after discontinuation of the drug. Palatability and convenience of use were rated high by the caregivers, who administered the drug daily to the horses during the study (Orsini et al, 2012).
Despite a long history of use, the mechanism of action of paracetamol is still not fully understood.
It is considered to be a weak prostaglandin inhibitor with analgesic and antipyretic effects that are largely centrally mediated, where inhibition of prostaglandin E2, substance P and 5-HT3 receptors occurs (Graham et al, 2013). Effects via cannabinoid pathways have also been described (Sharma and Mehta, 2014).
Paracetamol (20mg/kg orally twice daily) has been described for adjunctive analgesic use in a case of laminitis (West et al, 2011) with poor response to other analgesic medications, including NSAIDs and opioids.
A recent study has demonstrated the safety of paracetamol administered at 20mg/kg via multiple oral dosing over a 14-day period (Mercer et al, 2019).
Licensed oral preparations of paracetamol are available for dogs (in combination with codeine) and pigs in the UK, although no specific equine product is available.
Gabapentin is used in human medicine for the management of neuropathic pain and as an antiseizure medication. It has been used in horses for the management of neuropathic pain – such as trigeminal neuritis and femoral neuropathy – with some success (Davis et al, 2007).
It can be administered IV or orally; however, oral bioavailability is low (Terry et al, 2010), which may limit its usefulness outside a hospital setting.
Oral doses reported include 2.5mg/kg at intervals of 8 hours, 12 hours or 24 hours (Davis et al, 2007), and 2mg/kg to 3.3mg/kg at intervals of 8 hours or 12 hours (Dutton et al, 2009).
Efficacy is largely judged by improvement of clinical signs – for example, improvement in head shaking frequency or severity, and improved pain scores. Behavioural effects include some sedation, as well as polydipsia, and are more commonly associated with IV use.
Limited literature is available for the duration of treatment, and this will depend on the disease process. In the case report by Davis et al (2007), post-anaesthetic femoral neuropathy was treated for six days with gabapentin, although more protracted courses may be required for head shaking.
Tramadol is a synthetic analogue of codeine, which is used in the management of acute and chronic, moderate to severe pain in humans.
It acts centrally with agonist activity at μ opioid receptors, and inhibits the reuptake of noradrenaline and serotonin.
No equine licensed product is available, although the pharmacokinetics and pharmacodynamics of IV, IM and orally administered tramadol have been investigated (Giorgi et al, 2007; Shilo et al, 2008; Dhanjal et al, 2009; Stewart et al, 2011; Knych et al, 2012).
Evidence exists in human patients of significant individual variability in drug efficacy, and it is thought drug metabolism is largely genetically predetermined (Giorgi et al, 2007; Knych et al, 2013).
Equine oral bioavailability is reportedly between 65 per cent and 85 per cent higher in fed horses (Giorgi et al, 2007) when given at a dose rate of 5mg/kg orally twice daily, although, similarly to in humans, significant individual variation exists in plasma concentrations.
IV administration in horses has been associated with some side effects – including ataxia, muscle twitching, sweating, tremors and tachycardia – at dose ranges between 2mg/kg and 5mg/kg (Giorgi et al, 2007).
Although evidence exists of efficacy, clinical use is not yet commonplace and further investigation is warranted before routine use can be recommended.
Since a high prevalence of developmental and degenerative joint diseases are present within the equine population, intrasynovial analgesia offers an attractive and effective method for targeting pain relief.
Several drugs are commonly administered by this route – including morphine, which is perhaps most useful in the perioperative period where surgical treatment has been provided; and corticosteroids, which are commonly used with success in the management of degenerative joint diseases.
A review of intra-articular medications is beyond the scope of this article; however, this route of medication will often contribute significantly to overall patient comfort, having given due consideration to potential associated risks and accepting not all patients will be good candidates for all therapies.
Accurate evaluation of pain in horses is of fundamental importance to animal welfare and for effective veterinary management of equine patients (Viñuela-Fernandez et al, 2011).
Physiological parameters alone – such as changes in heart rate or respiratory rate – are inadequate in quantifying or identifying changing pain states in animals (Bussières et al, 2007).
Pain scales have been developed using several behavioural and physiological parameters that have been identified to increase in magnitude, or frequency, in horses experiencing pain. These scales include, but are not limited to:
In a clinical setting, Dutton et al (2009) described the use of composite multifactorial pain scoring in the management of hoof pain, and found the method facilitated the recognition of a changing pain state and the subsequent alteration of therapy.
More recently, the subtle behavioural changes in horses associated with pain have been investigated and may be reflected in changes in facial expression.
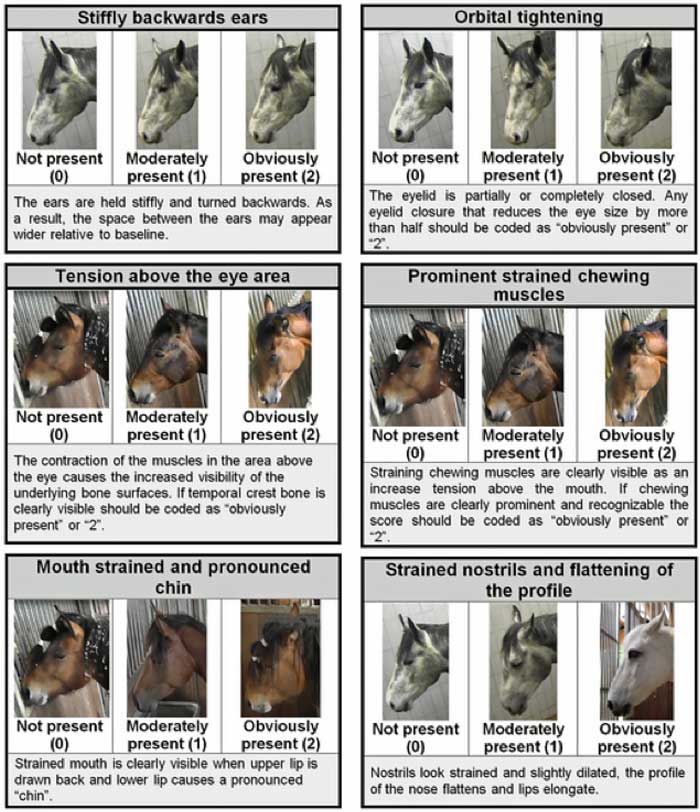
The Equine Pain Face has been described by Gleerup et al (2015) in horses subjected to acute somatic pain, and the Horse Grimace Scale has been described by Dalla Costa et al (2014) when they investigated the pain face of horses undergoing routine castration (Figure 1).
Although the evidence relating to the most effective analgesic options in horses may be behind that of other veterinary species and the human medical literature, continuing efforts must be made to optimise the analgesia we offer to horses.
Application of our knowledge to the field situation is possible and our aim should be to advance our knowledge in a way that benefits our patients, both in the hospital and field settings.
A growing body of literature exists in equine analgesic options, and with the improved awareness and increased application of pain scoring methods, our analgesic care of our equine patients should continue to improve. In 2005, only 36.9 per cent of UK equine veterinarians provided analgesia following castration (Price et al, 2005).
Hopefully, with increasing awareness of equine pain behaviours and more data regarding the use of analgesics in horses, this under-treatment will have improved (McFadzean and Love, 2018).