3 Dec 2018
Christian Byrne and Safia Barakzai present a case of a cob mare diagnosed with this uncommon finding, then discuss general diagnosis and treatment.

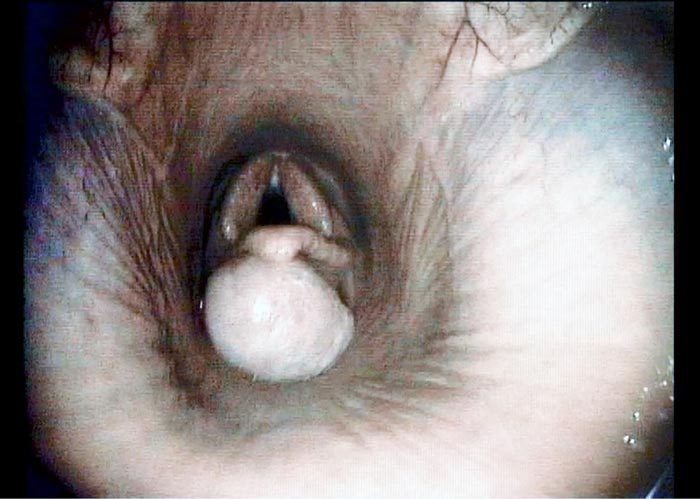
Figure 1. A videoendoscopic image demonstrating the large subepiglottic cyst at presentation. Note the secondary elevation of the epiglottis.
Subepiglottic cysts are an uncommon finding in equine practice and their aetiology has not been completely elucidated. Signalment, history and clinical examination findings are variable, and this article discusses a case that presented with nasal discharge and coughing when eating.
Endoscopy often demonstrates the subepiglottic cyst with a degree of epiglottal elevation. Surgical excision is the most common treatment and can include conventional surgery via a laryngotomy, or minimally invasive techniques in standing sedated or anaesthetised patients.
Transendoscopic excision is performed by nasal or oral approaches, and can be undertaken using a laser or a snare. The long-term outcome following surgical excision is generally excellent, with a low rate of recurrence.
A 13-year-old cob mare kept as a pasture pet was presented for investigation of coughing, which had been present for approximately six weeks and was getting more severe.
The owner reported coughing was most severe while the mare was eating forage. Onset of coughing also coincided with the development of mild, mucopurulent nasal discharge from the left nostril. A course of antimicrobial therapy resulted in a temporary resolution of nasal discharge.
Clinical examination confirmed the mare to be systemically healthy, with vital parameters within normal limits. Mild, left-sided, mucopurulent nasal discharge was evident, though no coughing during examination. Facial symmetry was normal, with no external evidence of dental disease. No evidence of lymphadenopathy was present and auscultation of the lung fields was normal.
Prehension is the initiating step of ingestion and is followed by mastication within the oral cavity. Following formation of a bolus in the caudal oral cavity, swallowing is stimulated.
This involuntary process involves constriction of the pharynx progressing the bolus beyond the relaxed cricopharyngeus muscle into the oesophagus.
The bolus is then propelled by primary and secondary peristaltic action of the oesophagus to the stomach.
Coughing associated with eating is most commonly an indication of impairment of deglutition in the pharyngeal or oesophageal phases. Differential diagnoses for these include:
A unilateral nasal discharge is typically associated with upper respiratory tract disease rostral to pharynx (including the ipsilateral sinuses, nasal cavity and, occasionally, the guttural pouches).
However, exceptions do occur, with Dixon et al (1995) having reported 3.3% of cases with primary pulmonary disease had a history of only unilateral nasal discharge.
In this case, endoscopy of the upper respiratory tract was elected as the primary diagnostic procedure. This demonstrated a large (approximately 3cm diameter) well demarcated, mucosa-covered mass positioned ventral to the epiglottis and the epiglottic cartilage was dorsally deviated by the mass (Figure 1). A diagnosis of subepiglottic cyst was therefore made. Endoscopy of the trachea showed a small amount of food material on the tracheal walls. No abnormal respiratory secretions could be seen emanating from the sinus drainage angle on the left side.
Standard radiographic projections of the paranasal sinuses were also performed in this case due to the history of unilateral nasal discharge. No abnormalities were noted. It was assumed the nasal discharge was due to the low level of aspiration of food and tracheitis present.
The mare was treated with transendoscopic laser excision of the subepiglottic cyst. The mare received perioperative antimicrobial (procaine penicillin 20mg/kg IM) and NSAID (flunixin meglumine 1.1mg/kg IV) therapy.
Standing sedation was achieved with romifidine hydrochloride (40µg/kg IV) and butorphanol tartrate (10µg/kg IV). Lidocaine hydrochloride was transendoscopically applied topically to provide local anaesthesia of the subepiglottic tissue and both nasal passages.

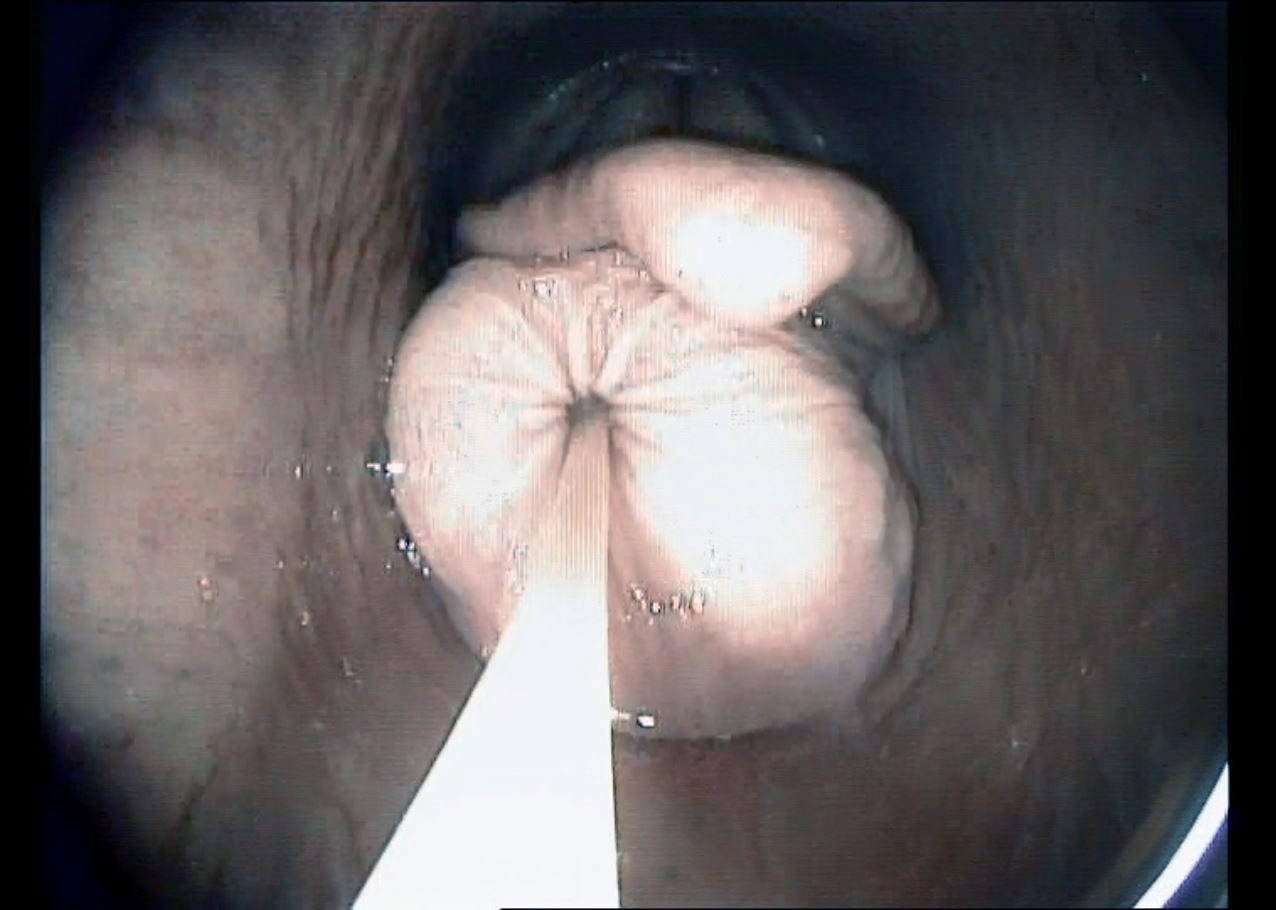
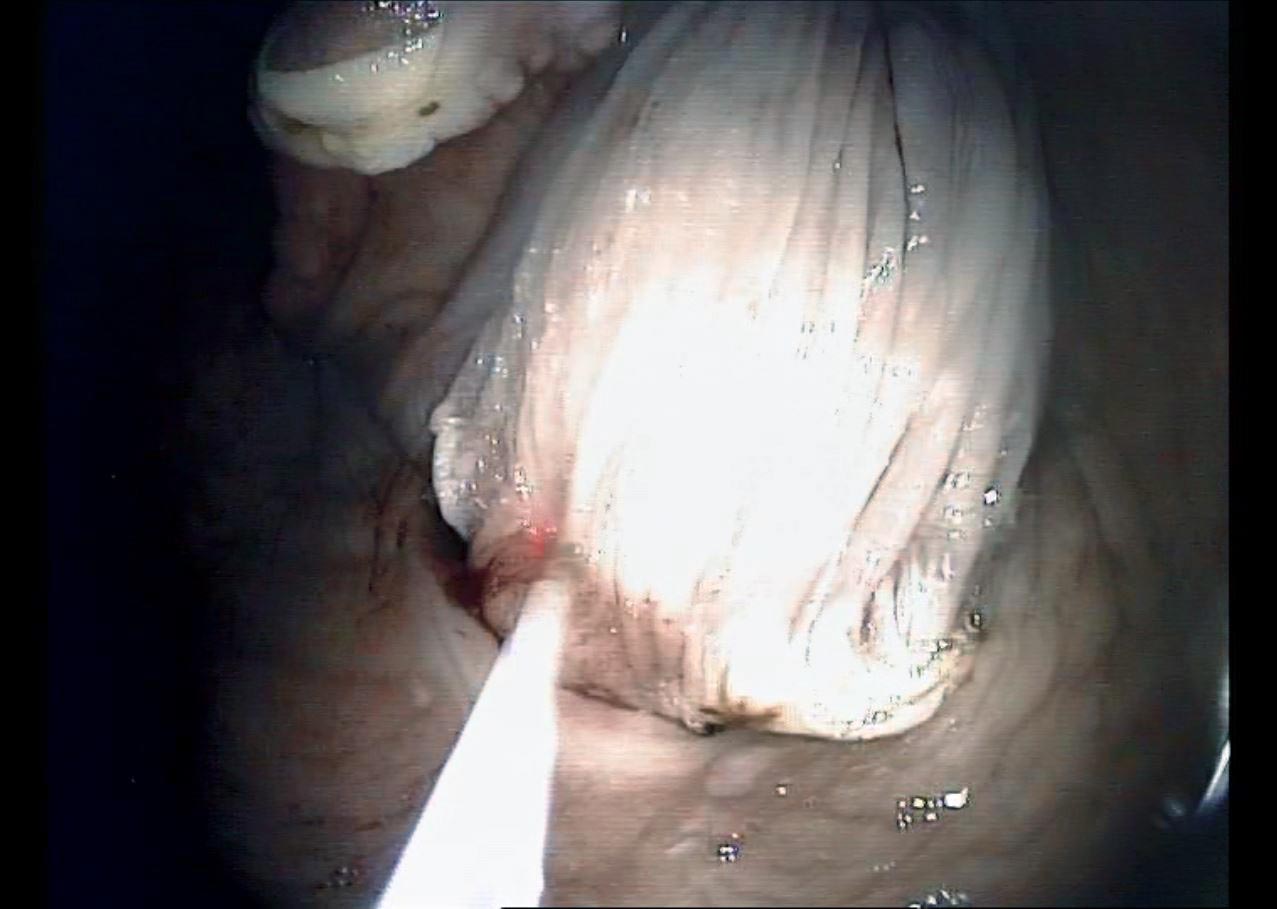
A transendoscopic lance was used to penetrate the cyst and aspirate approximately 15ml of serous fluid (Figure 2). This partially deflated the cyst, easing manipulation and assisting in dissection. With endoscope in situ, curved bronchoesophageal grasping forceps were passed through the contralateral nasal passage and used to manipulate the cyst (Figure 3). A transendoscopic diode laser was used to excise the cyst en bloc, along with the overlying subepiglottic mucosa using a contact technique (Figures 4 and 5). Following excision, topical dexamethasone sodium phosphate (total 20mg) was applied to the surgical site.
One day postoperatively, repeat endoscopy was performed, demonstrating moderate inflammation of the subepiglottic tissue, which is to be expected following a procedure of this nature. Transendoscopic topical dexamethasone treatment was repeated.
The mare was discharged from the hospital one-day post-surgery, with a course of phenylbutazone (2.2mg/kg by mouth twice a day for five days then 2.2mg/kg by mouth once a day for a further five days), with a two-week period of rest. The mare was re-presented five days postoperatively following an episode of suspected overexertion when turned out in a small field. Marked inflammation of the subepiglottic tissue was managed with temporary tracheotomy, antimicrobial and anti-inflammatory therapy and this reduced over a further four to five days.
Histopathology performed on the excised tissue confirmed it was a subepiglottic cyst – the wall consisted of well-vascularised and focally inflamed fibrocellular tissue, and the (empty) cavity was partially lined by ciliated columnar (respiratory) epithelium.
Subepiglottic cysts are an uncommon finding in horses (Aitken and Parente, 2011; Salz et al, 2013). Previous studies have compared equine subepiglottic cysts to thyroglossal duct cysts in human patients, implicating a developmental aetiology (Kelmer et al, 2007); however, in horses, they appear to occur in a variety of ages of animal. Histopathology has demonstrated varying epithelial linings (Davenport-Goodall and Parente, 2003; Aitken and Parente, 2011). The aetiology of subepiglottic cysts has not been fully elucidated, and these lesions may result from both developmental and acquired mechanisms (Davenport-Goodall and Parente, 2003).

Clinical signs and history are variable, and often relate to the breed and athletic activity of the horse. In adult horses, clinical signs are consistent with peri-epiglottal pathology, and may include coughing, nasal discharge, dysphagia, increased respiratory noise, poor performance and even syncope (Tulleners, 1991; Hay et al, 1997; Aitken and Parente, 2011). In Thoroughbred yearlings, subepiglottic cysts may be identified on routine endoscopy, with no abnormalities evident on routine clinical examination (Salz et al, 2013).
This case presented with coughing during eating and nasal discharge, most likely related to aspiration of food material and secondary tracheitis. The mare was a pasture pet and it is probable, in the authors’ opinion, that, had she been exercised, she would have exhibited abnormal respiratory noise.
Endoscopy of the upper respiratory tract typically confirms the presence of the cyst, although the cyst may be intermittently positioned ventral to the soft palate, making observation more challenging (Aitken and Parente, 2011).
The epiglottis is often elevated dorsally and further abnormalities, including epiglottic entrapment, may be present (Salz et al, 2013). Some cases of subepiglottic granuloma, may appear similar to a cyst (Fulton et al, 2012).
Endoscopy by mouth (with a full mouth speculum in place) and radiography of the larynx may provide further information (Davenport-Goodall and Parente, 2003). Some authors advocate direct palpation by mouth in some cases (Fulton et al, 2012).
A wide range of surgical treatments have been reported for subepiglottic cysts. The important principles of surgical management are to ensure complete removal of the cyst and limit excision of normal subepiglottal tissue, with the surgical site left to heal by secondary intention (Tulleners, 1991; Davenport-Goodall and Parente, 2003).
Most cysts can be excised using a routine laryngotomy under general anaesthesia (Fulton et al, 2012) – where the epiglottis is retroverted into the laryngotomy incision to access the subepiglottic tissue. Minimally invasive techniques using a cyst snare or transendoscopic laser are popular and can take an oral or nasal approach (Salz et al, 2013; Cramp et al, 2014; Parente, 2014).
As in this case, transendoscopic diode laser excision can be performed via a nasal approach in the standing sedated patient. Successful treatment by transendoscopic intralesional injection with formalin has also been reported (Dougherty and Palmer, 2008).
As with other upper respiratory tract procedures, using laser, collateral thermal damage and postoperative inflammation are important considerations (Ahern and Parente, 2008). Cases of subepiglottic cyst excision typically involve dissection of a relatively large section of tissue, which may predispose to increased postoperative inflammation.
The adjacent epiglottic cartilage should be vigilantly avoided. Healing of the subepiglottic surgical site following excessive tissue excision may result in an abnormal, ventral deviation of the epiglottis (Cramp et al, 2014). This can alter the relationship between the soft palate and epiglottis, and lead to persistent dorsal displacement of the soft palate (Davenport-Goodall and Parente, 2003).
This mechanism is comparable to the development of dorsal displacement of the soft palate following correction of epiglottic entrapment, which has be reported to occur in 10% of cases (Tulleners, 1991).
Long-term athletic outcome following complete surgical excision is excellent for both conventional and minimally invasive techniques, with a low risk of recurrence (Salz et al, 2013). Salz et al (2013) also reported 73% of horses performing their intended use following subepiglottic cyst excision (with some cases not performing due to unrelated problems).