21 Apr 2020
Aoife Ryan BVetMed, MRCVS and Matt Gurney BVSc, CertVA, PgCertVBM, DipECVAA, MRCVS discuss the medications commonly used by practitioners, as well as the induction of patients and future possibilities.

A practical guide to equine field anaesthesia has been discussed recently in veterinary literature (McFadzean and Love, 2017; Kruger, 2019).
The aim of this article is to discuss the pharmacology of drugs commonly used in equine field anaesthesia, to further practitioners’ understanding and facilitate appropriate drug choices. Anaesthesia of the adult horse will be discussed mostly.
It should be noted donkeys metabolise drugs differently to horses, partially due to their differing body water distribution. As a general rule, donkeys require 1.5 times the bodyweight dosing of a horse, although it is advisable to dose for a horse bodyweight initially and titrate upwards if required.
It is well documented that equine anaesthesia carries a significant risk to the patient. With this in mind, where possible, sedation and locoregional techniques should be considered to avoid some of the risks associated with general anaesthesia, such as induction and recovery.
Safety of personnel involved should always be paramount in the attending veterinary surgeon’s decision to sedate or anaesthetise a patient.
A premedication with good effect is paramount in facilitating a smooth induction, and may still be effective in the recovery period, dependent on the drugs used and duration of the procedure.
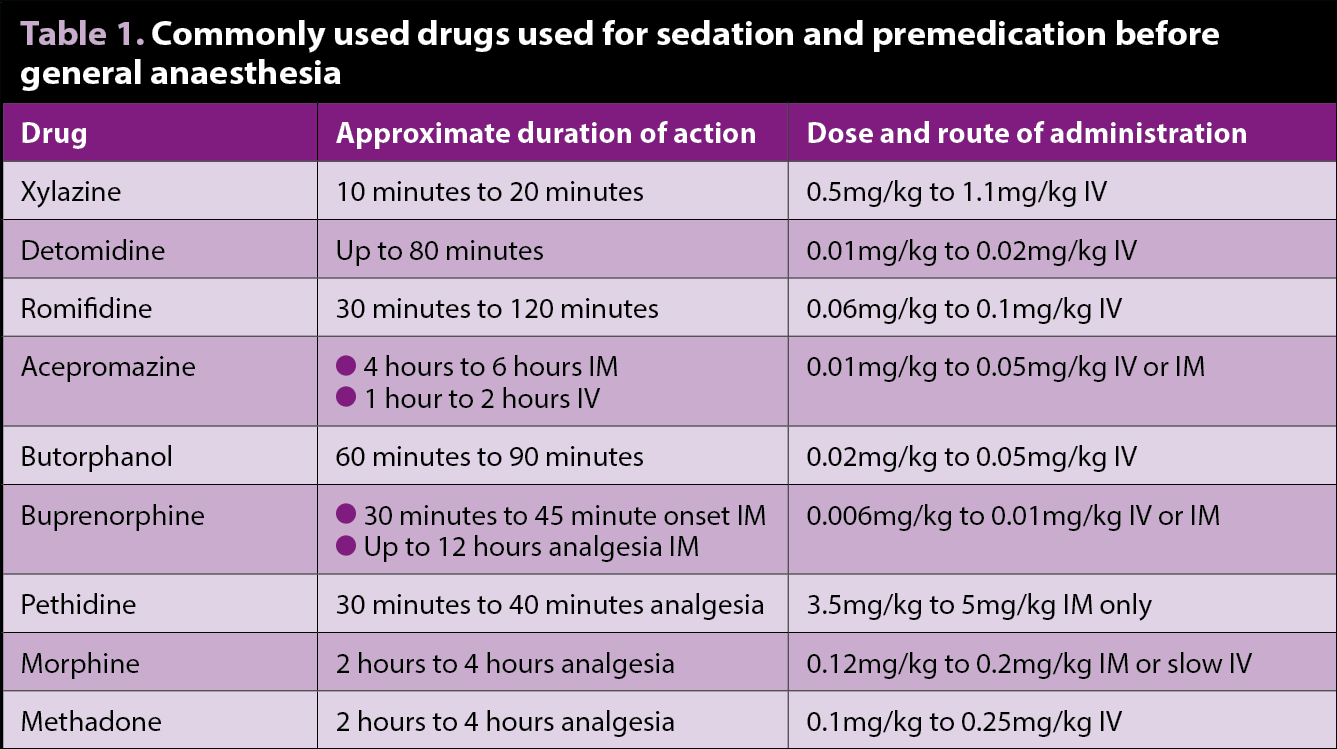
Table 1 lists drugs commonly used for sedation and premedication, as well as their approximate duration of action, and dose and route of administration.
Adrenoceptors are widely located throughout the body. They are activated by the neurotransmitters epinephrine and norepinephrine, and classified into two major groups of alpha (α) and beta (β) adrenoceptors.
Numerous subtypes of both α and β adrenoceptors exist, of which only α-2 will be discussed in this article.
Α-2 adrenoceptors can be further subdivided into α2A, α2B and α2C, and are found on primary afferent terminals at peripheral and spinal nerve endings in the dorsal horn of the spinal cord, brainstem and in vascular smooth muscle.
Stimulation of these receptors by α-2 agonists produce peripheral and spinal analgesia, sedation, peripheral vasoconstriction and inhibition of insulin secretion, leading to increased urine production. Side effects include bradycardia, arrhythmias, decreased cardiac output, respiratory depression, sweating and reduced gastrointestinal motility (Zullian et al, 2011).
Care should, therefore, be taken in the administration to critically ill patients, such as those with blood loss or cardiovascular compromise. Conversely, anxious horses or those with higher circulating catecholamines may require increased doses.
The most commonly used licensed α-2 agonists used in UK equine practice are xylazine, detomidine and romifidine, although dexmedetomidine and medetomidine are commonly used in small animal practice and can be used off licence in horses.
Xylazine is the shortest acting of these (10 to 20 minutes) and useful to provide sedation for short procedures, such as examination for colic.
Detomidine has a slightly longer duration of action (30 to 60 minutes) – sublingual formulations can be administered by owners and may provide sufficient sedation to allow procedures, such as clipping and dentals. Care should be taken in the administration of detomidine to colics in the field, as it is possible its longer duration of action may mask signs of deterioration (Jochle et al, 1989).
Of the UK licensed α-2 agonists, romifidine provides the longest duration of action (60 to 90 minutes) while producing less ataxia and a higher head carriage (England and Clarke, 1996) – making it useful for standing procedures or shoeing. It is frequently used as a premedication prior to general anaesthesia.
Opioid receptors – mu (μ), kappa (κ) and delta (δ) – are found peripherally, spinally and supraspinally.
Opioids can be categorised according to their agonist, partial agonist, agonist/antagonist or antagonist activity at these receptors. They provide analgesia by direct inhibition of the ascending transmission of nociceptive information from the dorsal horn of the spinal cord, and activate pain control circuits descending from the midbrain through the rostral ventromedial medulla to the spinal cord.
Administration of opioids in horses can be controversial due to the fear of side effects (Price et al, 2002), such as compulsive eating behaviour, box-walking and incoordination.
Opioids enhance the sedative and analgesic effects of α-2 agonists, and this combination can minimise the excitatory effects of the former.
Butorphanol – a κ receptor agonist and μ receptor antagonist – is the most commonly used opioid in equine practice, and most often used in combination with an α-2 agonist to provide sedation; combining them allows reduced doses of both drugs to be administered.
Buprenorphine, a partial μ agonist licensed for use in horses, has been found to provide superior analgesia to butorphanol for elective surgical procedures under general anaesthesia (Taylor et al, 2016).
Furthermore, a study comparing buprenorphine and butorphanol for field castration in ponies found buprenorphine to provide superior analgesia (Rigotti et al, 2014) – this should be considered when performing this procedure in the field.
Full μ receptor agonists produce the most antinociceptive effect, of which only pethidine is licensed for use in horses in the UK and is useful for analgesia for spasmodic colic.
Although not licensed, morphine and fentanyl are both listed as being essential for the treatment of Equidae for analgesia in Directive 2001/82/EC of the European Parliament – meaning they can be used in horses intended for food, providing a withdrawal period of at least six months is observed.
The administration of morphine can be controversial to some, due to a study identifying it as a risk factor for postoperative ileus and colic (Senior et al, 2004); however, a recent literature review found no strong evidence to suggest that perianaesthetic morphine increased the risk of colic (Mackenzie, 2017).
Methadone is licensed in small animal practice and can be used off-licence to provide analgesia.
The most commonly used phenothiazine used in veterinary medicine is acepromazine, which has been associated with a reduction in perioperative equine mortality (Johnston et al, 2002).
Both injectable and oral formulations are available – the latter can be useful for procedures such as loading for transport or clipping.
The anxiolytic effect of acepromazine is mediated by its antidopaminergic actions on the CNS. Antagonism at peripheral α-1 adrenoceptors results in vasodilation and hypotension; therefore, caution should be exercised in hypovolaemic patients or those with cardiovascular compromise. Vasodilaton can also lead to hypothermia.
Priapism has been reported; therefore, traditionally acepromazine has not been used in stallions (Dugdale, 2010).
Acepromazine has both a long onset and duration of action – animals should, therefore, be left undisturbed for at least 30 minutes following administration.
Response to acepromazine can be unpredictable, both between patients and on an individual basis. Its actions can be potentiated by the co-administration of an opioid. Combining acepromazine with α-2 agonists for premedication before general anaesthesia can improve haemodynamics (Marntell et al, 2005).
Before induction of general anaesthesia, horses should be well sedated. Signs of appropriate level of sedation include minimal response to sound, a low head carriage and a drooping lower lip.
Ketamine is a non-competitive antagonist at N-methyl D-aspartate receptors and is commonly used in combination with a benzodiazepine (Wohlfender et al, 2015) to induce anaesthesia following sedation with an α-2 agonist (ketamine 2.2mg/kg to 3mg/kg IV; benzodiazepine 0.05mg/kg to 0.1mg/kg IV).
Ketamine produces a rapid onset and short duration of dissociative anaesthesia (10 to 15 minutes). Care should be taken with repeated bolusing, and sufficient time should pass before recovery from anaesthesia (15 to 20 minutes) to ensure a good-quality recovery. The addition of an α-2 agonist, such as xylazine, can be beneficial in this case to provide sedation for recovery.
Due to its sympathomimetic action, ketamine maintains – and can improve – cardiac output and blood pressure. If given alone, it can be excitatory and causes poor muscle relaxation.
Ketamine maintains cranial nerve reflexes, and has both analgesic and anti‑inflammatory properties. It can be infused at subanaesthetic doses as part of a multimodal approach to analgesia in managing both acute and chronic pain, although excitation can occur at higher doses.
Benzodiazepines (diazepam and midazolam) exert their action by enhancing the activity of gamma-aminobutyric acid, the primary inhibitory neurotransmitter of the CNS.
They are used in combination with ketamine to induce anaesthesia, and have been found to improve induction quality, ease of intubation and surgical conditions, while not negatively impacting cardiovascular parameters or recovery quality (Allison et al, 2018).
Benzodiazepines are useful in foals, and can be used alone to induce recumbency or combined with ketamine for short anaesthetics.
Following a ketamine/benzodiazepine co-induction, anaesthesia can be maintained with repeated bolusing of ketamine at between a third and a half of the induction dose as required, or at 10-minute to 15-minute intervals.
If xylazine has been administered in the premedication, xylazine should be administered at half the original dose in the subsequent ketamine top-ups.
If detomidine has been administered, a further half-dose of detomidine should be administered between 20 minutes and 30 minutes after the original dose. Romifidine can be given at 25 per cent of the original dose as required (Clarke et al, 2014).
Guaifenesin is a centrally acting muscle relaxant and can be used as part of a “triple drip” recipe (plus an α-2 agonist and ketamine) for procedures shorter than 90 minutes. This is because guaifenesin accumulates in tissues, which can lead to ataxia in recovery.
Because of this risk of accumulation, it is advisable not to include guaifenesin in the induction protocol and use for maintenance of anaesthesia only.
It should be noted guaifenesin is not analgesic and is extremely irritant if administered extravascularly; therefore, care should be taken to ensure correct catheter placement.
Donkeys are particularly sensitive to guaifenesin and should be dosed with care, as they can become apnoeic and hypotensive following administration (Bidwell, 2015).
Monitoring during the use of this drug combination can be difficult as horses can appear “light” due the ketamine in the infusion – this can result in the infusion rate being increased when, in fact, the horse is in a deeper plane of anaesthesia.
Infuse at 1ml/kg/hr to 2ml/kg/hr, reducing infusion rate after 30 minutes to avoid accumulation
The recommended triple drip recipe is detailed in Panel 1.
Alfaxalone is not licensed in the horse, but is used frequently in small animal practice. It can be used in horses in combination with benzodiazepines to induce anaesthesia, and is comparable to ketamine (Klöppel and Leece, 2011).
Following induction, anaesthesia can be maintained with boluses in a similar manner to ketamine, or used as an infusion (Deutsch et al, 2017).
A study investigating co-administration with medetomidine in colts for castration found surgical conditions to be adequate and recoveries to be of good quality (Goodwin et al, 2013).
Some drugs mentioned in this article are used under the cascade.