25 Jul 2016
Jonathan Anderson looks at how to diagnose whether the underlying cause for any particular horse's lameness is orthopaedic or neurological, including distinguishing the ataxic from the lame horse.
Jonathan Anderson
Job Title
Figure 6. 3D CT reconstruction of the equine cervical spine illustrating the synovial joint capsule and relationship with the nerve roots emanating from the ventral aspect of the vertebral body. Effusion of the joint capsule can result in impingement of the nerve roots, which at the level of C6 to T2 could result in gait abnormalities of the forelimbs.
Lameness or gait abnormalities in horses most commonly are due to underlying orthopaedic aetiologies, but neurological disorders can also be a significant cause of equine lameness conditions. In fact, in some causes of neurological disease, gait abnormalities in the horse may be the principal feature. This article will look at how to diagnose whether the underlying cause for any particular horse is orthopaedic or neurological, including distinguishing the ataxic from the lame horse.
Neurological causes of equine lameness may be overlooked unless they have some of the more common presenting features relating to specific nerves of the fore and hindlimb.

Peripheral neuropathies involving the radial, tibial, femoral, peroneal and sciatic nerves all present with distinctly recognisable features1. Likewise, shivers and stringhalt are likely to have an underlying neurological component, and a more detailed explanation of these conditions has also been covered1. Lameness or gait abnormalities in horses most frequently have underlying orthopaedic aetiologies, but in some cases of neurological disease, gait abnormalities can be the principal feature.
Distinguishing orthopaedic from neurologically related gait abnormalities can be a diagnostic challenge involving the use of multiple subjective and diagnostic modalities. Depending on the site of pathology, different gait abnormalities or clinical symptoms will be seen (Table 1).
The most common cause of neurological gait abnormalities in the horse is inflammation of the cervical spinal cord resulting from dynamic or static compression within the cervical spinal column. Cervical spinal cord compression can result in gait abnormalities. One of the most common is ataxia of both forelimbs and hindlimbs, resulting in these horses classically being termed “wobblers”.
This article will address distinguishing the ataxic from the lame horse as a means of determining if the underlying cause is orthopaedic or neurological.
Horses whose underlying lameness issues are related to neurological causes can have variable histories most commonly featuring an “irregularly irregular” gait abnormality2. Tripping and stumbling, intermittent low grade or marked lameness also may feature. In addition, wearing of the hind and (less commonly) the front toes, a hypermetric gait, poorly developed musculature (especially cervical and gluteal regions) and/or concurrent stiffness of the neck may accompany the gait abnormality being described.
Affected horses often have bilateral muscle atrophy especially affecting the cervical and gluteal musculature, as opposed to more asymmetric muscle atrophy associated with orthopaedic conditions2,3. Additionally, an intermittent, or changing, gait abnormality, an inconsistent pattern of the abnormality or a multiple-limb gait abnormality can indicate a proprioceptive deficiency, so careful neurological investigation is warranted (Figure 1).
Lameness investigations with the aforementioned historical and clinical features should also be neurological in nature. Lameness investigation relating to neurological issues usually requires orthopaedic assessment prior to the neurological causes being explored (Figure 2).
It is well recognised a horse’s neurological status varies from day to day and in different environments. Several examinations over different days and in different conditions (ridden, at home, at the hospital) are, therefore, recommended in cases where neurological symptoms are more subtle2. The neurologically affected horse has a reduced capacity, or an inability, to recognise the position of the trunk, pelvic and thoracic limbs and head in space – in other words, proprioceptive deficits. Horses with stenotic myelopathies resulting in gait abnormalities present with varying degrees of paresis (weakness), ataxia (incoordination) and dysmetria (exaggerated or reduced limb reflex inhibition).
Paresis may predominantly involve flexor or extensor muscle groups. Extensor weakness in a limb is best evaluated for muscle trembling, buckling on a limb when turning and the ease a patient can be pulled to one side either standing still or moving. Flexor weakness is evident as toe dragging, low foot flight and stumbling, especially while turning.
Ataxia results in varying degrees of abnormal foot placement, such as truncal sway during walking, placing feet out of line from one step to the next, crossing the limbs over each other when turning, pivoting on the inside limb when turned in a tight circle and weaving of the affected limb during swing phase of the stride3. Specific functions of the nervous system can be challenged in a neurological horse to try to exacerbate the aforementioned signs3. These include walking with the head elevated, walking up and downhill, backing up, turning in tight circles and moving around or over obstacles.
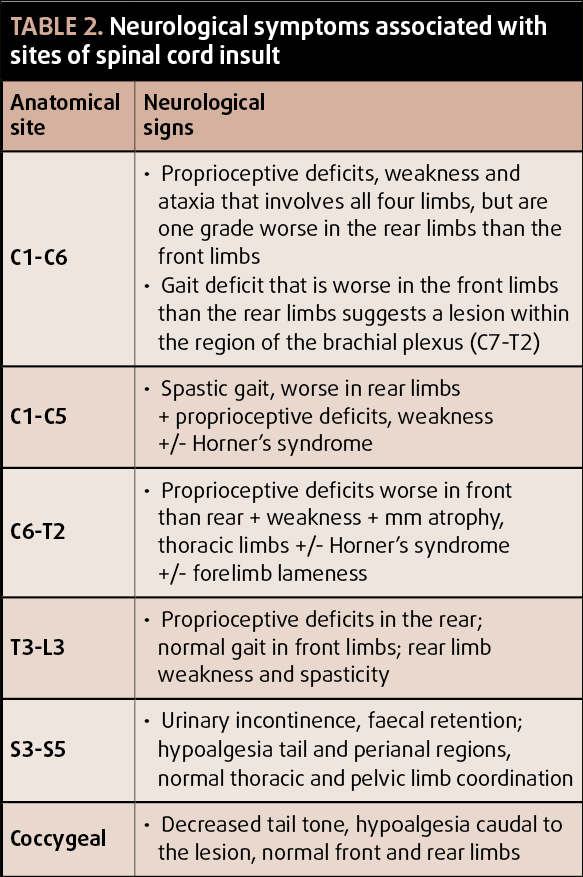
Ataxia will often be seen in changes of speed and direction; for example, abduction of the hindfoot when turning at the end of a trot or adoption of a basewide stance when stopped. Some or all of these can be used to determine the neurological status of the horse and a neurological grade can be assigned to the horse, as outlined in (Table 2)2.
![Figure 1. A diagnostic flowchart relating to clinical signs to specific regions of the nervous system. (Adapted from Furr M and Reed S [2008]. Equine Neurology, Blackwell Publishing Professional).](https://testing-vettimes-next.sfo3.digitaloceanspaces.com/2016/08/VTE2.2-Anderson-Figure-1.png)
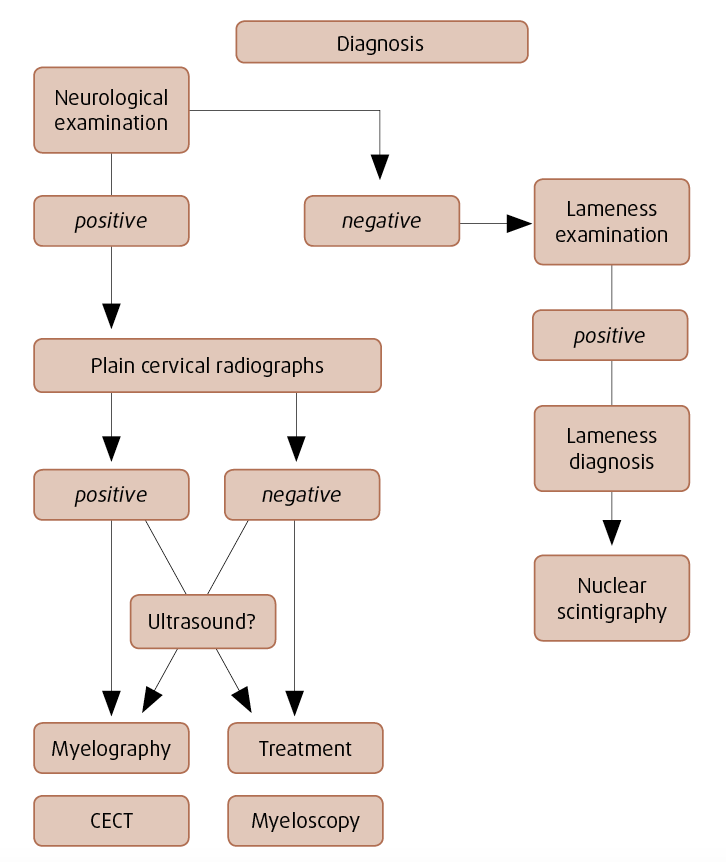
Although a lame horse will typically have a full lameness assessment performed prior to cervical issues being investigated, horses with more subtle gait abnormalities, or the more non-specific signs already outlined, are more likely to benefit from nuclear scintigraphy. This includes the cervical spine as a means to investigate regions of interest and determine involvement of the appendicular skeleton.
While nuclear scintigraphy is highly sensitive for bone remodelling it can be difficult to interpret in the cervical region. Articular process joints that have increased radiopharmaceutical uptake in one site or side greater than the contralateral site or side are worthy of radiographic investigation. Cervical radiography allows assessment of the articular processes and associated joints between vertebrae, from the occiput to the junction of C7 and T1.
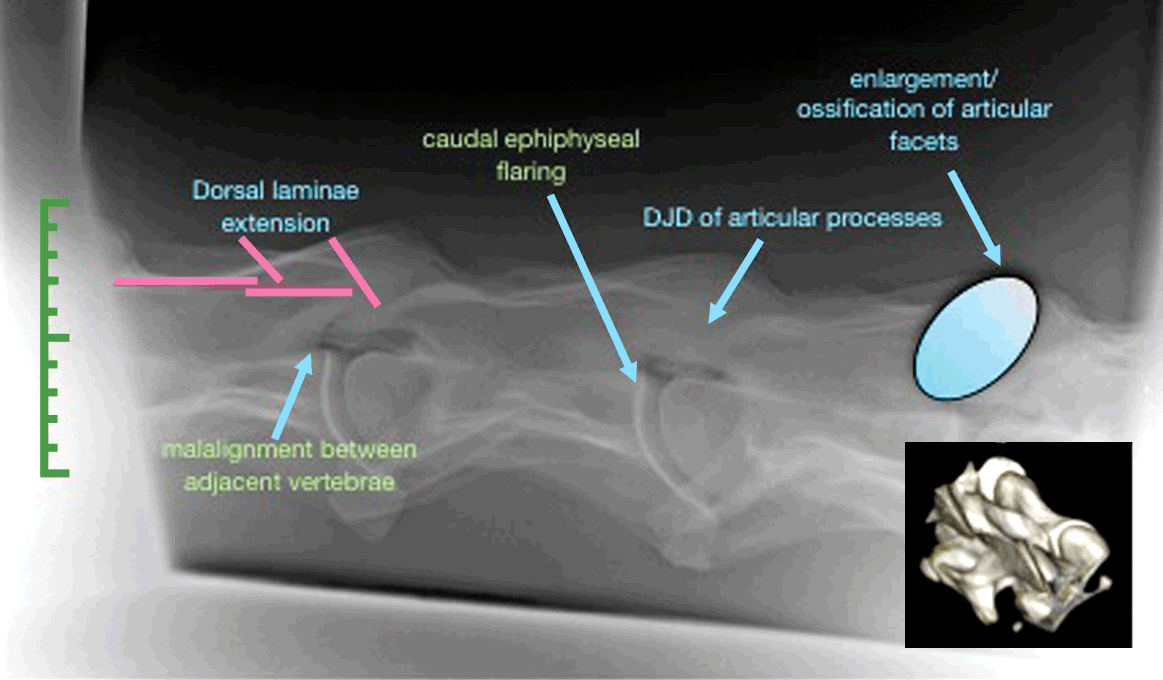
As well as lateral views taken from both sides, 30° proximal-lateral to lateral-distal oblique views aid in identification of specific abnormalities affecting one side over the other. Typically, changes associated with cervical vertebrae stenotic myelopathy (CVSM) are seen between C5 and T1, with developmental abnormalities in young horses (younger than four) seen in the mid-cervical region (C3/4)2. Five radiographic changes evidence vertebral pathology (Figure 3). These are dorsal extension of the laminae, malalignment of adjacent vertebrae, caudal epiphyseal flaring, osteoarthrosis of the articular processes and enlargement/ossification of the articular process2.
Caudal cervical articular process pathology has been classified radiographically with varying degrees of dorsal and ventral new bone formation affecting the articular process joints. However, these have not been correlated with severity of clinical disease4. That being said, significant remodelling of the cervical vertebral joints can result in neurological symptoms associated with compression axially of the spinal cord or with lameness if the remodelling of
bone is lateral and compression of the nerve roots associated with the one limb5.
Ataxia has been attributed to two broad classifications of cervical spinal cord compression. Cervical static stenosis describes compression of the cord, irrespective of the degree of flexion or extension of the neck, and is usually attributed to remodelling changes associated with cervical articular process6.
Cervical vertebral or spine instability (CSI) describes the dynamic compression that occurs with malalignment of the vertebral canal between adjacent cervical vertebrae, which varies in severity depending on the position of the neck and that is usually attributable to conformational abnormalities or fractures of affected vertebrae6. While typically the latter condition affects young horses and results in ataxia, mild compression can result in more vague signs, such as muscle weakness, consistent training difficulties (related to difficulty in schooling correctly through to persistent upward fixation of the patella), or inability to canter united.
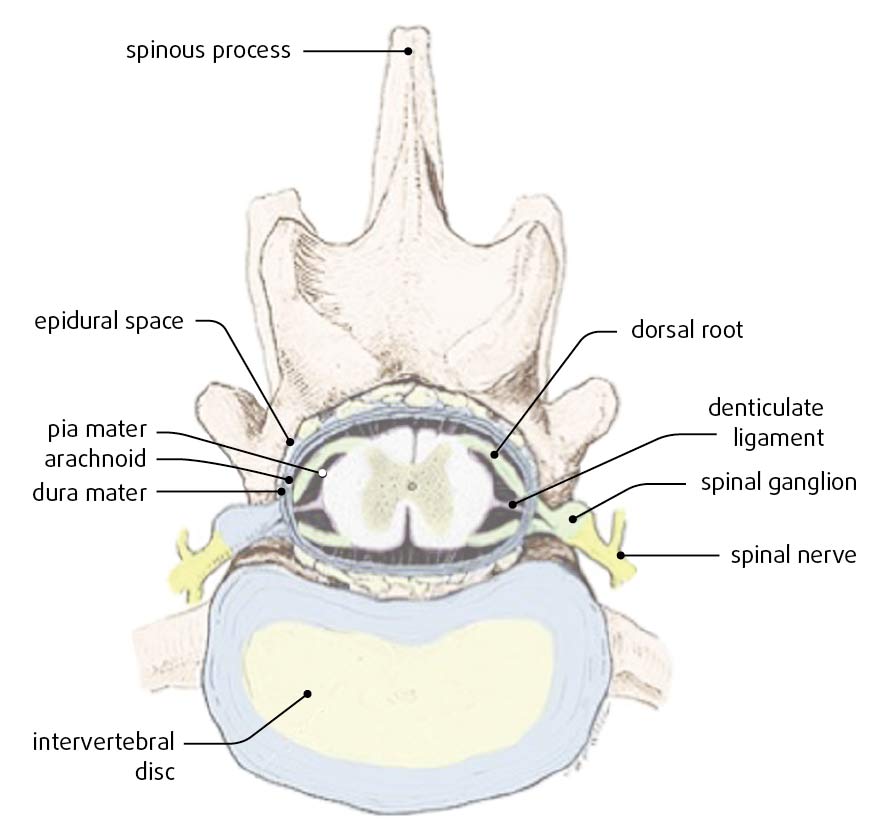
With CVSM, abnormal growth patterns lead to a spinal canal that is narrowed, or that becomes narrow when the neck moves and the vertebrae move relative to each other7. This, in turn, leads to compression of the spinal cord. The spinal cord white matter is compressed initially, resulting in damage to the ascending general proprioception pathways (ataxia) – that is, the sensory pathways that enter the white matter by way of the dorsal root – and the descending upper motor neuron pathways (paresis), namely the ventral root pathways2 (Figure 4).
As compression is prolonged, damage progresses deeper through the white matter. Because the pelvic limb proprioceptive tracts emanate more superficially than those of the thoracic limbs, pelvic limb movement is affected more frequently and more severely2 (Figure 5). The degree of severity of clinical signs is related to the degree of compression or remodelling associated with the cervical vertebrae.
![Figure 5. Schematic of the spinal cord illustrating the superficial position of the pelvic limb spinocerebellar tracts compared to the thoracic limb equivalents. This helps to illustrate why the hind end is so often clinically affected in cases where spinal cord compression is a feature. (Adapted from Nout YS and Reed SM [2003]. Cervical vertebral stenotic myelopathy, Equine Vet Educ 15[4]: 212-223).](https://testing-vettimes-next.sfo3.digitaloceanspaces.com/2016/08/VTE2.2-Anderson-Figure-5.png)
While ataxia may be a feature of CSI as well as cervical static stenosis (CSS), the latter commonly presents as stiffness of the neck or unilateral lameness that can be marked in its severity. CSS can also present as poor performance issues, poor musculature and weakness, disunited cantering through to severe lameness issues affecting forelimbs unilaterally or bilaterally5. Typically, such investigations start as lameness evaluations with the cervical spine becoming the place of last resort to find the issue once other regions have been eliminated from the investigation by blocking and imaging.

The brachial plexus that supplies the nerve supply to the forelimb emanates from C6 to T2 vertebrae, and C6/C7 and C7/T1 are most frequently involved with osteoarthritis, making the pressure on the nerve roots from new bone formation and inflammation of the synovial capsule a common sequelae (Figure 6).
Therefore, horses with muscle atrophy in the mid to distal neck – with a history of a stiff neck and displaying lameness that cannot be regionalised to the limb – should be considered likely candidates for cervical radiology and nuclear scintigraphy to establish the involvement of the cervical vertebrae and associated structures. In a study this year, an idiopathic hopping-like lameness has been described where nerve root compression from cervical spinal cord inflammation has been implicated8.
These horses have a characteristic lameness seen under saddle, with the affected forelimb on the outside of the circle varying in its severity and frequency. The “diagnosis” is one by exclusion, although in two such cases in this author’s experience, myelographic examination indicated compressive lesions that may reflect the impression of the joint capsule of the affected articular process joint (Figure 7). The synovial capsule of each cervical articular process joint has been eloquently mapped, demonstrating they extend no greater than 2mm into the vertebral foramen and become progressively bigger the more caudal in the neck they are located9.
In a diseased joint they can result in sufficient medial extension to result in spinal cord impingement9. Laterally, the joint capsule is closely associated with the nerve roots, and thus effusion of the joints laterally can result in nerve compression with resultant forelimb lameness or paresis.
Radiographic evidence of articular process joint remodelling, in conjunction with the already outlined historical and clinical symptoms and complemented with increased radiopharmaceutical uptake on nuclear scintigraphy, provides sufficient reason to pursue treatment directed towards alleviation of inflammation in the region.

Ultrasound may be used to confirm the presence of increased synovial fluid within the joint and remodelling of the articular processes, although – in the author’s opinion – this is highly subjective unless there are obvious differences one side over the other at the same site10. It is most useful as a means to perform accurate placement of anti-inflammatory medication into the joint.
Myelography allows confirmation of suspicious minimal sagittal diameter ratios on plain cervical radiographs that may be resulting in compression of the spinal cord on a dorsal-to-ventral, but not lateral-to-lateral, orientation11.
Up until recently it has been the gold standard for diagnosing spinal cord compression5,6. While it has a relatively high specificity (83%), it has a low sensitivity (56%). This means if the horse has a positive finding on myelography, it likely has the disease, but only 53% of affected horses will have a positive myelogram2 (Figure 8). This makes it a poor gold standard diagnostic test. In the author’s opinion, it remains an essential component of neurological evaluation, as surgical treatment of horses with spinal cord compression carries a good prognosis, especially in horses with more subtle clinical evidence of gait abnormality. The myelogram is readily and easily performed and brings important diagnostic information to help make an informed decision about treatment and outcome.
A great deal of subjectivity remains in the correlation between clinical symptoms and imaging findings relating to the cervical spine. Additionally, the insensitivity of radiographic and myelographic imaging to identify early and more subtle changes means an early diagnosis and, therefore, appropriate treatment is delayed.
Therefore, as with many other areas of equine diagnostics, the gold standard to diagnose cervical spinal conditions lies in the use of advanced imaging techniques. Reports of both CT and MRI in cadaveric specimens detail the vastly superior degree of diagnostic information to be obtained of both bone and soft tissue in the cross-sectional plain. Study results of myelographic CT in 16 horses, identifying 14 lesions and achieving diagnostic images from C1 to T1 in three of them and to C7 in all horses, have been reported12.

Most equine hospitals in the UK with CT capabilities are limited to imaging down to C3 in either the standing or the anaesthetised horse, due to the diameter of the CT tube. Larger diameter CT tubes that enable identification of pathology to the level of C7/T1, as described by Kristofferson (2014), are in place or being constructed in three sites in the UK – Rainbow and Liphook equine hospitals and the RVC. This will massively enhance the ability to accurately diagnose pathology of the cervical spinal column and sites of compression, both on to the spinal cord as well as the spinal nerve roots, and, thereby, identify neurological causes of lameness.
The addition of myelographic contrast in CT myelography will enable superior diagnostic information to be obtained with respect to the influence of pathology on the spinal cord and leads to exciting possibilities for treating such lesions in new ways. It will become the gold standard way to confirm clinical suspicion of lameness/gait abnormalities that are a result of cervical pathology.
In summary, the investigation of the horse with lameness issues related to underlying neurological disease must include both orthopaedic and neurological examinations, in conjunction with good quality and complete sets of bilateral cervical radiographs, as a minimum.
Cervical radiographs can be difficult to interpret and correlate with clinical symptoms, and, therefore, examinations on different days, different surfaces, and by more than one clinician may help to obviate bias and error.
Myelography is important to distinguish evidence of spinal cord compression, but the use of CT myelography offers the most exciting means to diagnose pathology accurately, and lesion-orientated treatment, therefore, becomes more plausible and site-specific.