23 Sept 2019
Jamie Prutton and Fleur Whitlock discuss recent confirmed outbreaks of this respiratory virus in horses, along with surveillance, classification, vaccination protocols and biosecurity.

Equine influenza (EI) is a highly infectious respiratory virus that is endemic in the UK (Panel 1).
During 2019, laboratory-confirmed outbreaks had reached 216 distinct foci in the first seven months of the year, with each outbreak potentially involving many horses with clinical signs. With an anecdotal estimate that only 30% to 40% of the equine population is vaccinated against influenza, it should not really be a surprise that the spread of this virus has been more extensive across the UK this year.
All Florida clade 2 viruses between 2010-17. Evidence of continuous Florida Clade 2 circulation in UK since large outbreaks in 2003 (Nkt/5/03).
Virological analysis confirmed the strain implicated in recent outbreaks is Florida clade 1 – a strain that has not been responsible for a large number of outbreaks in the UK for more than 10 years.
The increase in EI activity in the UK led to the closure of the racing industry for a short period, as well as numerous shows being cancelled and properties being placed on lockdown, to reduce the spread of disease. EI has a limited infectious period (less than or equal to 10 days) and no carrier state, and relies on chains of transmission. Prevention and control strategies are aimed at breaking these chains. Vaccination is fundamental to prevention and control. By raising the level of immunity in a group, the virus quickly runs out of susceptible animals to infect and propagate as an onward transmitting outbreak.
The recommendation for six-monthly boosters was made in January, following an increase in EI activity in the UK and Europe. Changes have been made to vaccination recommendations to attempt to reduce the rate of spread, and the clinical severity of disease in the population and individuals, respectively.
These changes started prior to the 2019 outbreaks due to an increased activity of EI in the UK in 2019, compared with 2018, and increased European activity, but have been solidified through this year. The financial threat of this disease can be highlighted by the billion dollar cost to the Australian equine industry in 2007 following the outbreak there.
Clinical signs are detailed in Panel 2.
Most people are fully aware of the clinical signs, but they include:
Signs may be mild in vaccinated horses and equine influenza should be suspected in any vaccinated case demonstrating non-specific respiratory signs. Following infection, horses are more susceptible to other opportunistic infections and, therefore, should not be placed under extra pressure or stress during the 50 to 100 days following clinical infection.
Disease surveillance in the UK is maintained by the World Organisation for Animal Health (OIE) reference laboratory at the AHT. A fast diagnosis is necessary to limit spread and the Horserace Betting Levy Board (HBLB) supports a surveillance scheme, enabling free laboratory testing of suspect clinical cases.
This scheme was established to enable epidemiological and virological monitoring of viruses implicated in UK outbreaks and select epidemiologically relevant strains for inclusion in vaccines. The information is then disseminated through a number of channels, including online (www.equiflunet.org.uk), on Twitter @equiflunet and via SMS with Tell-Tail, sponsered by Boehringer Ingelheim (www.telltail.co.uk).
Sampling should include both a nasopharyngeal swab and paired bloods not less than 14 days apart. Horses that should be tested can include:
The clinical case being examined may not be the best choice for sampling by nasopharyngeal swab, and a more acutely affected unvaccinated in-contact would be ideal. Mass swabbing of yards is discouraged and, ideally, two or three horses with signs can be tested.
An article by Durham (2019) reviewed the pathogenesis, antigenic drift and immune response, and how these pertain to the vaccine choices available to the practising vet.

The classification of EI is based on subtype, the location and year of isolation. Two glycoproteins – haemagglutinin and neuraminidase – are essential to the pathogenesis of the virus. These glycoproteins are prone to antigenic drift, enabling this virus to evade host immunity, and leading to difficulty for the immune system to respond appropriately and for vaccinations to be kept up to date. The different lineages and sublineages of the virus are depicted in Figure 1, which also highlights when those strains were, or are, circulating within the UK.
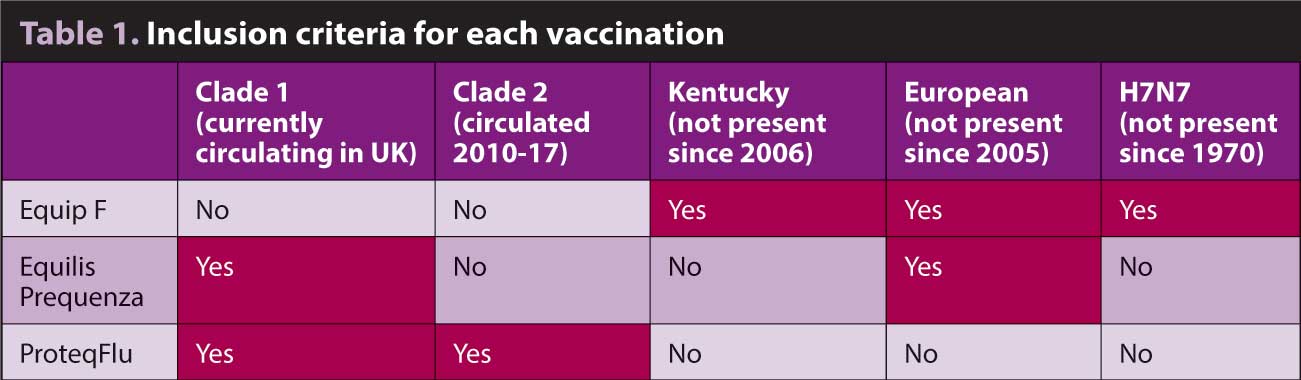
The importance of the lineage information and current outbreaks is highlighted when considering which vaccine is to be administered. Within the UK, three licensed products are available for vaccination against EI, although they are all quite different (Table 1).
As can be seen from Table 2, only ProteqFlu (Boehringer Ingelheim) currently conforms to the OIE-recommended clade 1 and 2, while Equilis Prequenza (MSD Animal Health) conforms to the OIE-recommended clade 1. Equip F (Zoetis) only fulfils the OIE guidelines from 24 years ago (which remained unchanged until 2004) regarding the lineages that should be present in each vaccination.
The OIE guidelines are produced annually in response to the circulating EI strains and should represent a guide for manufacturers to work towards. The current OIE advice is based on the 2010 recommendations, although during the meeting in April 2019, it stated its recommendations “are currently unchanged from those made each year since 2010”.
It went on to further state: “It is not necessary to include an H7N7 virus or an H3N8 virus of the Eurasian lineage in vaccines as these viruses have not been detected in the course of the most recent surveillance and are, therefore, presumed not to be circulating. Vaccines should contain both clade 1 and clade 2 viruses of the Florida sublineage.”

During the first seven months of 2019, 216 laboratory confirmed outbreaks around the country have occurred. An outbreak is defined as a discrete foci of infection – usually a premises – which may involve one or many animals with clinical signs. As can be seen from Figures 2 and 3, a fluctuation in the number of outbreaks per month has occurred, with June accounting for just less than a third of all outbreaks in the year so far.
The reason for the sustained increase in numbers since April is likely associated with the increased movement and mixing of horses through the late spring and summer months. Alongside the official events, a number of events exist where vaccination is not required, with a distinct increase in numbers of cases occurring in late June following Appleby Horse Fair.
Infection in vaccinated animals has been confirmed for all three UK vaccine brands, and of the 216 confirmed outbreaks, 25 have involved cases of flu in vaccinated horses. Reasons for diagnosing flu in vaccinated horses was multifactorial:
Therefore, breakdowns in cover have occurred, with both the OIE 2010 recommended vaccination and the OIE 2004 recommended vaccination. It is important to state occurrence of disease does not categorically mean a failure of the vaccination – rather, we should consider the population medicine of vaccination rather than solely the individual. As such, the likely decreased shedding duration and severity will have decreased the risk of spread to other horses.
When considering the vaccination protocol, the datasheet of the chosen product should be followed, even though the numerous regulatory bodies allow for larger windows for primary course administration, contrary to the datasheet recommendations. Due to the increase in EI activity in 2019, changes in the frequency of boosters have been recommended to ensure optimal immunity is maintained.
Fédération Equestre Internationale (FEI) continues to recommend boosters within 6 months and 21 days of a competition following completion of the primary course, and that no vaccinations should take place within the 7 days prior to arrival at a competition. Currently, all three vaccination products are permissible under FEI rules.

The British Horseracing Authority (BHA) has stated that, as of 1 May 2019, all horses have to show they have been vaccinated within the past eight months (plus a one-month grace period) to comply for racing. They have also proposed that, as of 1 January 2020, all horses will need to have vaccinations every eight months. No vaccinations should be given on the day of the race or the six days prior to racing. Currently, all three vaccination products are permissible under BHA rules.
Often, the problem arises at shows where vaccination for attendance is not required and, ideally, the basic guidelines should be followed when running a show:
Although all professional bodies have not agreed on definitive vaccination protocols, it is advisable to recommend more frequent vaccinations than the current annual booster. We know vaccinations lessen the severity of the disease and duration of shedding of the virus in the individual animal. More importantly, though, it will reduce the spread of the virus through the population.
Therefore, even if an owner feels it is unnecessary for his or her horse to be vaccinated more regularly, it would be wise to discuss the population medicine, as well as the individual approach.
The AHT has proposed a streamlined mandate for vaccinations, which each individual organisation will need to decide whether to adopt. The following are the proposed new harmonised vaccine dosing intervals, with appropriate justifications.
The use of vaccinations is imperative in the control of EI, but excellent biosecurity is also essential to reduce the spread, reduce the rate of occurrence and protect the remainder of the population. Biosecurity measures will be dictated by location, but advice for owners when going to an event should include:

The other high-risk period is the introduction of new horses to a property – especially if their vaccination and clinical history are unknown. To try to reduce the risk of EI occurring, the following should be followed.
Many of the yards experiencing EI outbreaks during 2019 had clear risk factors identified for the source and subsequent spread of infection. These included unvaccinated horses, recent new arrivals, mixing of horses at equine events and large yards with mixed vaccination status populations. The majority of affected premises did not adopt a vaccination policy, or apply a biosecurity plan on or off the home premises, and had no protocols for new arrivals.
The increased EI activity in the 2019 outbreak has highlighted the vulnerability of the population to EI and the requirement to continue vaccinating – ideally at an increased frequency for the majority of the population. No reduction in the rate of new cases appears to exist as we go through the summer months, but, hopefully, this will occur as the number of shows decreases and, more importantly, the vaccination uptake remains increased.
Time will tell if the virus manages to adapt beyond vaccine capabilities (antigenic drift in the current circulating strain versus a completely new strain). That is where ongoing sampling of suspect cases and submission of these samples on the HBLB scheme is essential.