3 Jul 2017
Gayle Hallowell looks at developments in the diagnosis and treatment of this condition.
Gayle Hallowell
Job Title
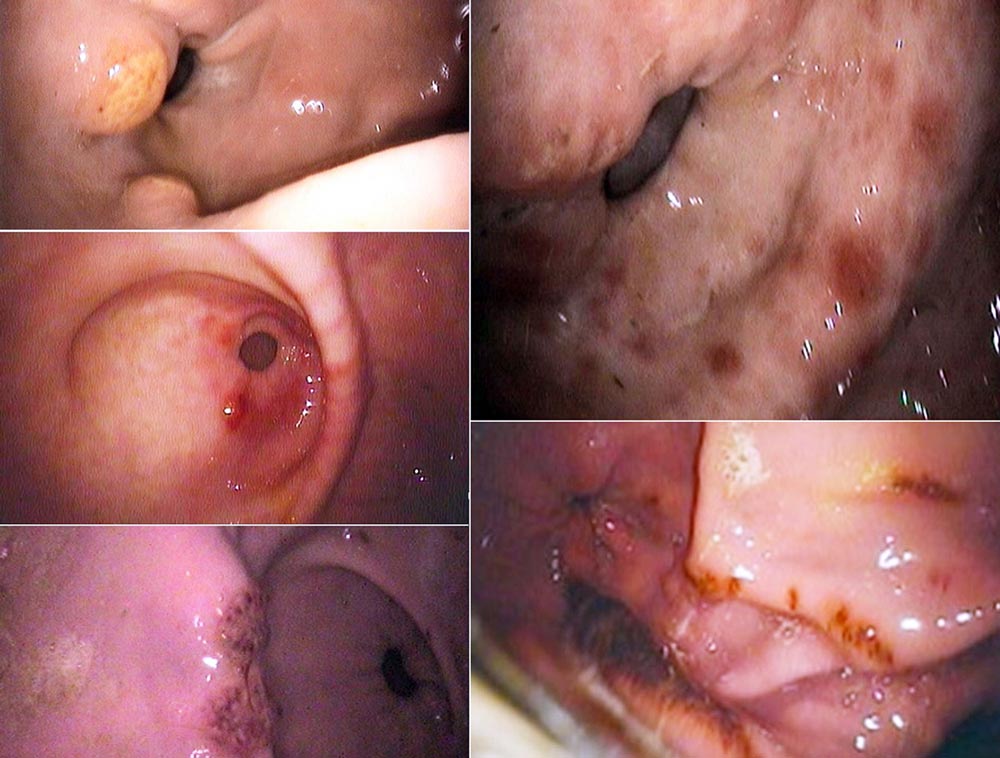
Figure 3. A collection of images showing a range of glandular lesions that can be identified with gastroscopy in the horse.
The prevalence of equine gastric disease is high and studies have suggested glandular disease is as prevalent, or more so, than squamous disease.

Studies have identified glandular lesions in 50% to 70% of racehorses, and leisure and sports horses. It is widely accepted disease of the squamous and glandular gastric regions are not the same, regarding pathophysiology, epidemiology and natural history, just as Habronema species and gastric squamous cell carcinoma are distinctly different.
Despite investigations of various tests, gastroscopy is still the mainstay for diagnosis. Little new information exists regarding squamous disease, except perhaps some data on alternative drugs and regimens shown to be successful. However, where glandular disease is concerned, it appears the more we learn, the more questions it raises. Some key publications in the past few years have evaluated success and failure of the conventional and novel treatments for gastric glandular disease discussed here.
Clinical signs associated with gastric disease are non-specific and unreliable to be used to diagnose the conditions discussed in this article.
Some investigations have attempted to find tests that can screen for gastric disease. These have included the succeed test aimed at identifying protein and blood in faeces. This test has shown to be ineffective, which is not surprising for two reasons. The first is significant bleeding is not seen in most cases of equine gastric disease. The second is as horses are hindgut fermenters, the bacteria in the colon are likely to break down blood and protein before the gastrointestinal contents are excreted. The second screening test evaluated has been the sucrose absorption test.
Preliminary data suggests this test is unreliable for use in adult horses, but has shown some promise as a screening test in foals. Therefore, the only diagnostic test suitable for the diagnosis of equine gastric disease is gastroscopy and, as this article will hopefully highlight, it is important to diagnose whether horses have squamous or glandular disease.
It is necessary to examine on every gastroscopic examination both the squamous mucosa and glandular mucosa in the pyloric region (Figure 1). Most lesions in adult horses are in the pyloric antral region. In some larger horses, a 3m gastroscope may not be long enough to enable evaluation of the pyloric antrum.
Various tips can be used to make examination of the whole of the stomach possible. The first is the horse needs to be appropriately starved. Some horses have slower gastric emptying than others, but usually 12 to 16 hours is sufficient. In the author’s experience, some gastric distension with air, but not too much, enables majority of the gastric mucosa to be evaluated. However, if too much air is instilled, it will push the pyloric antrum further away, making it more challenging to visualise. Once the stomach is appropriately distended, the gastroscope should be advanced along the greater curvature, the lesser curvature can then be seen and the pyloric antrum can be accessed directly below this (Figure 2).
The structure of these two gastric regions are different and the glandular region is designed to thrive in an acidic environment, whereas the squamous region is not. Is glandular disease a single entity or a syndrome, with multiple aetiologies? If this were a syndrome, it may explain the variability seen in response to treatment of this disease. Although we see a range of lesions (Figure 3), they do not appear to correspond with disease severity or likelihood of response to treatment.
The old equine gastric ulcer syndrome grading system of one to four still is used for squamous lesions, but has been abandoned for glandular lesions. The new consensus statement has replaced the glandular grading system with a series of descriptive terms. The first part describes the anatomical location of the lesions (cardia, fundus, antrum and pylorus – the latter two being the most common sites in the adult horse) and the second part describes the lesions: focal, multifocal or diffuse; mild, moderate or severe; flat and haemorrhagic, flat and fibrinosuppurative, raised and haemorrhagic, raised and fibrinosuppurative, depressed with or without a blood clot; and depressed and fibrinosuppurative. We are still unclear which lesions are the least likely to heal.

We are unsure as to the underlying cause of equine gastric glandular disease. Is it triggered by gastric acid, which seems unlikely due to the regions adaptation or does gastric acid contribute to the worsening of lesions when they have developed? Reduced gastrointestinal blood flow is likely to play a role in the pathophysiology of this disease, if we extrapolate data from other species.
In human patients and dogs, one common cause of gastric disease is Helicobacter species. Despite several studies, we still lack convincing evidence this is a cause in the horse. The other common cause of gastric disease in human patients and dogs is NSAID (and steroid) administration. Again, rationally, one would explain this to be a cause in the horse, but the few epidemiology studies investigating glandular disease have failed to identify this as the case.
Evidence from a histopathological study suggests disease of the glandular region is inflammatory in origin and may be an extension of inflammatory bowel disease. Disease in the glandular mucosa has shown to be proliferative and not truly ulcerative in nature. Although this disease manifests as lesions surrounding the pyloric antrum, histopathological changes can often be identified throughout the glandular region (Crumpton et al, 2015).
Identification of risk factors is lacking for equine gastric glandular disease, but they have consistently shown to be different from squamous disease. However, horses with glandular disease are likely to be performing at a higher level or working more – they are less likely to be lame, are calmer and are more likely to have weight loss secondary to reduced appetite.
Studies have continued to support the findings that omeprazole is an effective treatment for equine squamous disease and, in more than 85% of cases, lesions heal in 28 days. However, some have suggested 1mg/kg omeprazole (a quarter of the licensed 4mg/kg dose) is as effective for the treatment of equine squamous disease as 2mg/kg and 4mg/kg.
A study has suggested esomeprazole (not licensed in the horse) at 2mg/kg may be a more effective acid suppressant in horses receiving a high-fibre diet and may be a more appropriate treatment for the small number of horses that do not heal with omeprazole (Sykes et al, 2017). Another study showed misoprostol – a prostaglandin analogue licensed for the treatment of gastric disease in humans, but not horses – was shown to cause longer-lasting acid suppression than omeprazole (Sangiah et al, 1989).
When compared to equine squamous disease, healing of glandular lesions is inferior and often requires longer courses of treatment.
Several studies have shown the healing of glandular disease is poor with omeprazole monotherapy once per day. The reason for omeprazole being unsuccessful in healing these lesions may relate to its inability to increase gastric pH enough or for a long enough period of time. Alternatively, it may be due to this disease not being dependent on increased pH for healing. However, a long-acting omeprazole injection will soon be available in the UK that may allow for a more consistent degree of acid suppression not dependent on enteric absorption, which may be of value for the treatment of this condition – although it is yet to be evaluated in clinical cases.
Sucralfate, although known to be a poor “gastric bandage”, increases prostaglandin E (PGE) and thus improves gastric blood flow, as well as promoting re-epithelialisation by preventing degradation of fibroblast growth factor. This has been shown in one study to have improved efficacy in the improvement and healing (60%) of glandular lesions when compared with omeprazole alone (Hepburn, 2014), but no better in another study when combined with omeprazole (20% healing rates; Varley et al, 2016).
Misoprostol was shown in the 1990s to be more effective than omeprazole at increasing gastric pH in the horse. In addition, it too is known to cause an increase in PGE in a similar way to sucralfate, and thus increases blood flow. This drug, although not licensed, has been used in the horse historically for the treatment of right dorsal colitis and has been used in humans for the management of gastric disease. This drug does have to be handled with care due to its abortigenic effects and should not be used in pregnant animals.
A study has shown this drug is extremely efficacious, with healing achieved in 72% of cases, which was significantly higher when compared with combined omeprazole and sucralfate (20% healing rates). Loose faeces and mild colic have been rarely reported as side effects (Varley et al, 2016).
No evidence exists for the use of antibiotics for the management of this condition. Helicobacter species have not shown to be responsible for this condition, biopsies of lesions do not demonstrate a neutrophilic infiltrate and thus do not support their use and one study in clinical cases did not find the administration of antibiotics alongside omeprazole to be any better than omeprazole alone (Sykes et al, 2014). As such, the author feels, without evidence for their use in individual cases, this is antimicrobial misuse.
Esomeprazole at 2mg/kg is another potentially useful drug for the management of gastric disease. This drug has been shown to more effectively increase gastric pH, particularly when horses are fed a fibre-based diet, and if acid does plays a role in the pathophysiology of glandular disease, or simply slows healing, may play a primary or adjunctive role.
On the role inflammation may play in equine glandular disease, will it ultimately result that steroids are appropriate therapeutics for this disease? If the primary underlying disease process is due to reduced blood flow then its use would be contraindicated, but if this were an extension of inflammatory bowel disease it may indeed play a role. The author has used this class of drugs successfully in a small number of cases that have been unresponsive to other therapies.
Many nutraceuticals have been tested in relation to treatment and prevention of equine gastric disease. Pectin-lethicin compounds may play a role in prevention. This drug has been shown to increase total mucus concentration in the stomach, bind bile acids and protect against oxygen free radicals.
Sadly, inappropriate data analysis makes it challenging to assess any true efficacy of many of the other products. Bismuth subsalicylate has anti-inflammatory activity and some advocate its use, but it has not been specifically evaluated for efficacy in equine glandular disease as an adjunctive therapy. Corn oil has been advocated as a supplement for the management of glandular disease as it has been shown to increase gastric pH and PGE2 concentration, but no studies have demonstrated efficacy as an adjunct to other therapies for management of glandular disease in the horse.
The fact different types of treatment work in certain cases may support that glandular disease is a syndrome caused by a variety of aetiologies. Transendoscopic biopsies have not been shown to be effective in differentiating between different types of pathology in horses. Thus, trying to identify cases that will respond to the variety of treatments available requires further study.
For the dietary management of squamous disease, frequent, fibre-rich feeds are recommended. However, as we do not understand the underlying pathophysiology of glandular disease, we do not know what recommendations should be made, especially when data suggests fibre affects the efficacy of drugs used for treatment. This lack of understanding regarding pathophysiology also limits evidence on what we should advise regarding prevention in terms of management and therapeutics.
Evidence exists in human babies and foals that prophylactic acid suppression leads to gastrointestinal disturbances, including necrotic enterocolitis and diarrhoea, and can result in increased mortality. As such, the best way to prevent gastric disease in foals is to treat the underlying disease process and hypovolaemia and use sucralfate to improve gastric blood flow.
The same may be true regarding long-term acid suppression in adults. Acid is present in the stomach for a reason and, as such, trying to manage potential underlying causes is important to prevent recurrence.
Gastroscopy is still the mainstay for the diagnosis of gastric disease in the horse and diagnosis is important as treatment of disease in the squamous and glandular mucosa are not the same. Lower doses of omeprazole appear to be as efficacious as the licensed dose for the treatment of squamous disease. Once-daily oral omeprazole is ineffective for the treatment of glandular disease.
A study has found misoprostol to be more effective than combined sucralfate and omeprazole for the treatment of glandular disease. Evidence for adjuncts in the form of nutraceuticals is lacking (Varley et al, 2016).