21 May 2018
Liz Mitchell looks at how common conditions in the horse should be diagnosed and treated in first opinion practice.
Liz Mitchell
Job Title
The most frequently reported broad categories of disease syndromes recorded in the 2017 National Equine Health Survey1 were skin problems (31% of all syndromes recorded); lameness, including laminitis (23%); metabolic diseases (8.1%); eye problems (7.6%); gastrointestinal diseases (7.5%); and respiratory (5.9%).
This article will address the key presenting signs associated with skin problems, lameness, gastrointestinal disease and respiratory syndromes, detailing the common differential diagnoses and a suitable first line treatment approach when dealing with each of these syndromes prior to definitive diagnosis.
Medical general practitioners now use online patient-side searches for clinical signs and treatment protocols as standard.
However, in first opinion mixed and equine practice, despite the availability of various veterinary apps, it is still essential the initial assessment highlights the key clinical signs, and the clinician is aware of the common differentials for that presenting sign and can administer appropriate first aid treatment prior to any further treatment or investigation.

This initial treatment is often based on a presumptive diagnosis and the response (or lack of) will add to the evidence to assist a more definitive diagnosis.
Skin disease is most commonly characterised by pruritus, scaling, nodules or hair loss. The two most commonly reported skin diseases are Culicoides hypersensitivity (sweet itch) and dermatophilosis (mud fever), while other differentials that should be considered include atopy, urticaria, dermatophytosis, Chorioptes, lice (Damalinia equi) and sarcoids.
In some cases – for example, urticaria – the history, appearance and distribution of the lesions may lead to a definitive diagnosis (Figure 1) and specific treatment can be instigated immediately.
Many other cases exist where a specific diagnosis will require further diagnostic tests; early diagnostic testing is prudent to improve accuracy and prevent the cost of inappropriate non-targeted treatment.
Punch biopsies (8mm) taken from several sites for histopathology can be extremely useful to assist with the diagnosis of many skin diseases, including pastern dermatitis, urticaria, leukocytoclastic vasculitis, eosinophilic granuloma and hypersensitivity reactions.
Hair plucks and culture are the procedure of choice to identify dermatophyte, and scrapes or coat brushing can be used to identify Chorioptes. Intradermal skin testing is complex, but can provide valuable assistance in the diagnosis of hypersensitivity reactions.

The majority of skin cases may not need fist aid treatment prior to definitive diagnosis, with the exception of severe hypersensitivity and urticarial reaction, which will benefit from immediate treatment with systemic glucocorticoids to prevent severe self-excoriation. Owners should be made aware of the potentially infectious nature of some skin diseases – for example, dermatophilosis (Figure 2) and dermatophytosis – and advised of appropriate hygiene precautions.
Lameness is a common presenting sign in the general equine population, with a high proportion suffering one or more episodes of lameness per year1,2,3.
Lameness may be acute or insidious in onset and, as such, clinical signs range from a loss of performance to recumbency or the inability to bear weight. Numerous causes of lameness exist, including foot abscess, solar bruise, laminitis, tendon and ligament injuries, fractures, sepsis of a joint or tendon sheath, cellulitis/lymphangitis, joint disease and exertional rhabdomyolysis.
A comprehensive history is essential and will often provide valuable diagnostic information. Clinical examination of the lame horse should seek to identify the degree of lameness and which limbs are affected, the strength of digital pulses in all limbs, and the presence of any heat, pain or swelling of the structures of the limb.
The severely lame horse can often present a challenge and judging if one or more limbs are affected can be difficult – particularly as prolonged gait analysis in such a case is not recommended. Observation at rest, and a preliminary examination of all limbs and digital pulses, may provide helpful information on the likely site of lameness prior to observation at walk. Gait analysis should seek to identify the upward movement of the head or sacrum during placement of the lame limb. Placement on a hard surface may be associated with a softer sound, compared to the footfall of the other three legs.
Foot lameness is common in the equine population, with foot abscess the most likely cause of sudden-onset severe lameness. So, it is imperative careful assessment of digital pulses and application of hoof testers is conducted in all lameness cases (Figure 3). Practitioners should be mindful many horses have chronic or long-standing injuries their owners are not aware of and may be unrelated to the lameness condition.
If a fracture is suspected on the basis of clinical exam and history, radiography of the affected area can assist with diagnosis, and should be carried out without delay to indicate prognosis and appropriate first aid treatment (Figures 4 and 5). If sepsis of a joint or tendon sheath is suspected, synoviocentesis under aseptic conditions is indicated to assess the white blood cell count.
In a severe hindlimb lameness with no signs of inflammation or pain in the distal limb, a rectal examination and ultrasound examination of the wing of ilium can assist with diagnosis of a pelvic fracture.
Ultrasound examination can also assist with the assessment of tendon, ligaments, joints and surrounding structures, but in the absence of concerns about sepsis, these examinations need not be conducted immediately, and are often better delayed until after the acute phase.
Where the site of lameness is not clear, further investigation normally requires referral to a clinic for further workup. Nerve blocking of severe undiagnosed lameness in the field is not advisable due to risk of exacerbating the injury due to increased weight bearing.
If the cause of the lameness is diagnosed on initial examination, appropriate treatment and management specific for that condition should be instigated. In cases where a definitive diagnosis cannot be reached, appropriate first-line treatment might include box rest – with moderate coverage of bedding over the whole floor area, and food and water raised, as well as phenylbutazone at 2.2mg/kg (half dose) and reassessment at 12 to 24 hours for further diagnostics to assist with localisation of the lameness.




Gastrointestinal disease has been more frequently diagnosed in recent years, with a notable increase in the number of horses diagnosed with gastric ulceration. This is most likely due to our increased knowledge of the prevalence of the disease4,5,6 and range of presenting signs (including weight loss, colic, appetite reduction, poor performance and behavioural changes), as well as the widespread availability of diagnostic gastroscopy.
Acute gastrointestinal disease normally presents with colic signs (Figure 6), including rolling, sweating, scraping the ground, looking round at flanks and urinating frequently. More subtle signs of gastrointestinal disease include reduced appetite, restlessness, increased time spent recumbent and change in dropping consistency or frequency.
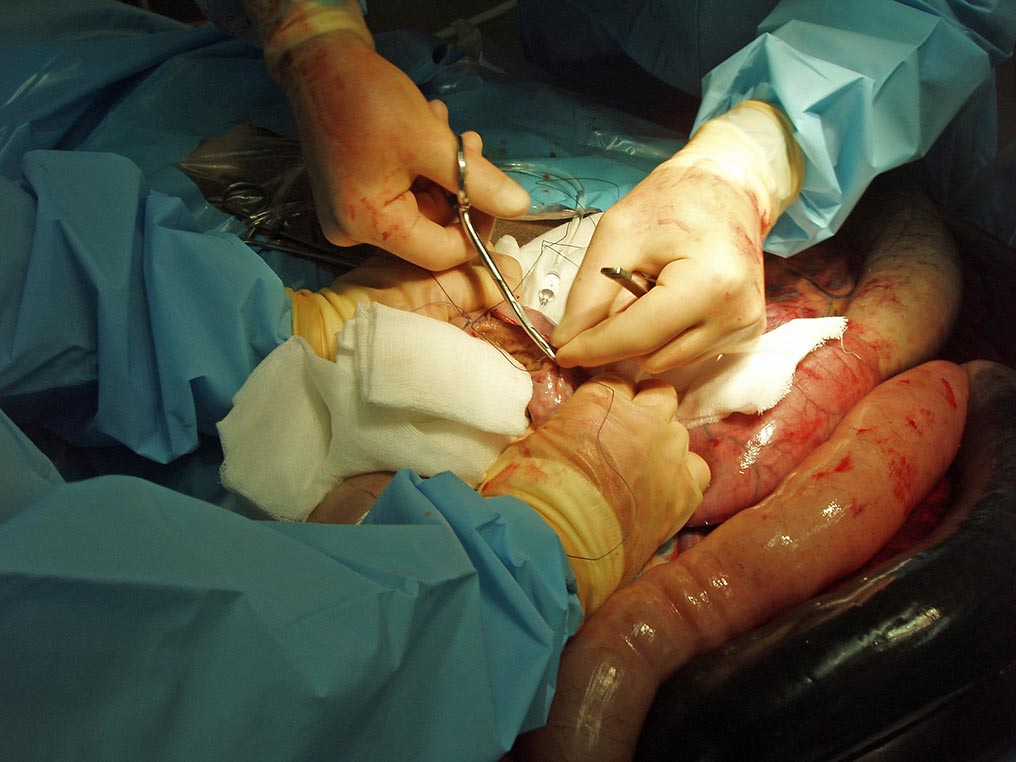
The vast majority of causes of abdominal (colic) pain can be successfully treated medically7 – for example, spasmodic (gas) colic, pelvic flexure impaction, colitis, cyathostominosis, enteritis and some colon displacements. Other causes may require rapid surgical treatment (Figure 7) – for example, strangulating lipoma, gastroepiploic entrapment, colon torsion, intussusception and some colon displacements. Some cases represent a hopeless prognosis at first presentation – for example, rupture of an abdominal viscus, severe endotoxaemia and acute grass sickness.
The goal of the first opinion practitioner in assessing a colic case is to quickly differentiate between these three groups to arrange rapid referral of surgical cases, appropriate treatment or referral for medical cases and rapid euthanasia of the hopeless cases.
Clinical assessments should be made on the degree of pain, mucous membrane colour, heart rate, respiratory rate, gut motility in all four quadrants and rectal temperature. Following the assessment of these parameters, the author favours the use of both hyoscine butylbromide (0.3mg/kg) and phenylbutazone (4.4mg/kg) prior to further diagnostic assessment, and the response to this initial analgesia is quantified and forms part of the diagnostic information.
Rectal examination provides valuable information, but may present a greater risk in small, young and poorly handled individuals. The use of low dose alpha-2 agonist and butorphanol will safely facilitate this in most patients; the prior use of hyoscine butylbromide also improves rectal relaxation.
The pelvic flexure, the region of the nephroplenic space, and position and distension of the abdominal viscera should all be palpated and assessed.
Passage of a nasogastric tube allows assessment of the degree, volume and nature of any gastric reflux. Increased reflux is associated with small intestinal obstruction, strangulation, enteritis or grass sickness. Abdominocentesis under aseptic conditions can assist in the identification of intestinal compromise.
Clinical findings consistent with medically manageable colic include heart rate below 60bpm, ingesta distended pelvic flexure and pain resolving following initial analgesia. In these cases, oral electrolytes may be administered by nasogastric tube, all food removed, and the patient closely monitored and re-examined if signs return or after 12 hours for further assessment if symptom-free.

Clinical findings consistent with surgical colic include heart rate above 60bpm, pain not responsive to initial analgesia, gas distensions of intestinal loops, gastric reflux and peritoneal fluid turbid or stained red/brown.
In these cases, analgesia to facilitate travel should be administered and immediate referral to a surgical facility arranged. In cases where surgery is not an option or in advanced cases representing a hopeless prognosis – toxic red/brown mucous membranes, unrelenting pain that can’t be controlled and evidence of ruptured viscus – immediate euthanasia on humane grounds should be carried out.
Respiratory disease, perhaps surprisingly, only accounted for 5.9% of reported veterinary problems in the 2017 National Equine Health Survey, although it is likely it accounts for a greater proportion of the first opinion equine clinician’s workload than this figure suggests.
The clinical signs of respiratory disease can include coughing, nasal discharge, dyspnoea, increased respiratory rate and depth, respiratory noise, poor performance and pyrexia. Initial clinical assessment should be made of breathing rate and pattern, heart rate, temperature and findings on chest auscultation.
Infectious respiratory disease will normally present with systemic illness and pyrexia, in addition to other respiratory signs; the common causes that should be considered are equine influenza, equine herpes virus, Streptococcus equi, Streptococcus zooepidemicus, Rhodococcus equi and Mycoplasma. Diagnosis should include nasopharyngeal swabs taken in the acute phase for virology and bacteriology, and paired serology. In cases of pneumonia, ultrasonography of the chest can assist with identification of pathology and diagnosis.
Prior to definitive diagnosis, NSAIDS should be administered, these cases put in strict isolation and the temperatures of in-contacts closely monitored (Figure 8).

Non-infectious respiratory disease is not normally associated with pyrexia or systemic illness, and clinical signs may include a loss of performance and increased respiratory rate and effort – and, in severe cases, dyspnoea. In dyspnoeic patients, it is important to differentiate inspiratory dyspnoea, indicating upper airway obstruction, and expiratory dyspnoea, indicating lower airway obstruction.
The common differentials for upper airway obstruction include sinusitis, retropharyngeal abscess and laryngeal paralysis secondary to, for example, hepatic insufficiency, botulism or lead poisoning. Severe cases should not undergo diagnostic endoscopy due to further obstruction of a compromised airway and, in these cases, first aid treatment involves tracheotomy.
Lower airway obstruction and disease may be caused by marked equine asthma (formerly called recurrent airway obstruction)8, foreign body obstruction and mild equine asthma (inflammatory airway disease)8. Endoscopy with tracheal wash and bronchoalveolar lavage will provide diagnostic information on the likely nature of the inflammation (Figure 9).
Prior to definitive diagnosis, the acute case may be treated with dexamethasone, atropine and furosemide. The response to atropine administration can aid in the diagnosis of marked equine asthma.
As first opinion clinicians we are faced with daily diagnostic challenges. A working knowledge of the key common differentials, employing appropriate diagnostic tests at an early stage and using prudent first aid treatment will assist in the satisfaction of a definitive diagnosis and targeted treatment.