14 Sept 2015
Tim Greet
Job Title
Figure 11. First appositional layer of mucosal closure using polyglactin.
A variety of intestinal anastomoses are used in equine surgery. This discussion will be restricted to those “end-to-end” anastomoses involving small intestine or “side-to-side” anastomoses between small intestine and caecum.

In some cases requiring anastomoses it can be difficult to correct the primary problem and thus carry out an anastomosis. Such situations include anatomical inaccessibility, when dealing with lesions of the duodenum or oral jejunum, or the aboral ileum.
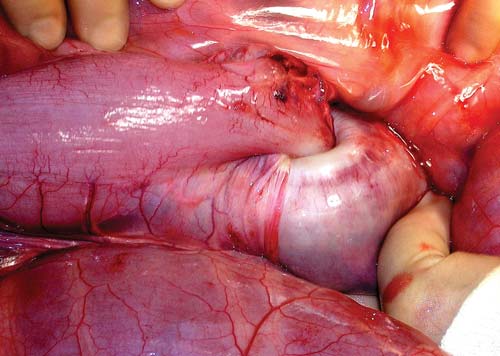
Fortunately, conditions demanding resection of the duodenum are very rare. Surgical procedures on the aboral ileum can be facilitated by using Lloyd Davis rectal occlusion forceps, with which the distal ileum can be grasped atraumatically (Figure 1), allowing some degree of leverage and therefore easier access.
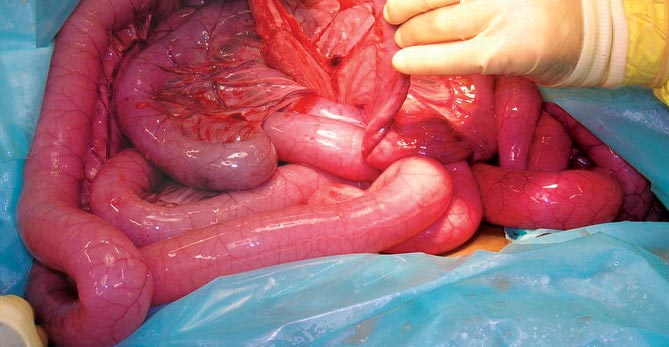
Resection of lengths of intestine much greater than 10m usually carries a poor prognosis, even though technically achievable; this is because of the inevitable endotoxic load that accompanies necrosis of this proportion of small intestine (Figure 2). Equally frustrating are those horses in which surgery is delayed and the intestine orad to the site of obstruction suffers irreversible compromise because of chronic distension, when earlier a short length of necrotic intestine might have been resected easily with a good outcome.
Sometimes, attempting to correct the primary problem has catastrophic consequences, such as fatal rupture of the portal vein when trying to retrieve small intestine incarcerated within the epiploic foramen. Experience teaches surgeons to be cautious when attempting this sort of manipulation and a variety of manoeuvres can be employed to assist in releasing the intestine. Patience is always a virtue in such cases and sometimes the apparently intractable lesion is eventually corrected quite successfully.
In some cases of intussusception, reduction may be very difficult or impossible. When short sections of aboral ileum are involved, the condition is often chronic and such lesions do not cause strangulation (Figure 3). In such a case a bypass ileocaecostomy without resection is effective. In jejunal intussusception, longer portions of intussusceptum may require to be resected in situ, as attempted reduction using force may result in intestinal rupture. Provided appropriate steps are taken to avoid peritoneal contamination this does not usually present a problem.


Surgeons should always be firm, but careful, when handling the intestine and its mesentery, particularly in young foals. In foals it is very easy to cause full thickness abrasion of the serosa of even healthy intestine, or a more serious injury if the mesentery becomes torn. Mesenteric tears can be sufficiently extensive to the point of creating a life-threatening defect, which cannot safely be repaired, and risking future intestinal incarceration (Figure 4). The use of copious volumes of sterile polyionic fluid and carboxymethyl cellulose can be very helpful when manipulating the intestine to reduce the risk of inadvertent damage.
Once the strangulated intestine has been released, it should be decompressed and then allowed 10 minutes “to recover”, allowing assessment of colour, motility and thus viability. It is sometimes quite astonishing to watch apparently devitalised intestine recover colour and motility, allowing the surgeon to avoid a time-consuming resection and anastomosis (Figures 5 and 6).

If it is clear the affected intestine is non-viable or even sufficiently compromised to the extent paralytic ileus would appear likely, a resection should be performed.
The author suggests the old adage of “if in doubt, cut it out” should probably be followed. Having said that, experienced surgeons are generally bolder in leaving questionable sections of intestine in situ, often with good results.
Over the years, a number of techniques have been used in an attempt to create a reliable and objective means of assessing intestinal viability, including oximetry, vascular ultrasound, fluorescence and intestinal biopsy. However, none of these have been found more practical or effective than subjective evaluation by an experienced surgeon.




Before attempting intestinal resection, it is essential to isolate the involved intestine from the rest of the peritoneal cavity using one or more sterile plastic drapes (Figure 7) and large sterile swabs or towels. It is important intestine is not allowed to dry out under the heat of operating lights and regular lavage with polyionic fluid is important. It is critical to identify exactly the extent of the segment to be removed, starting initially with the individual blood vessels that must be ligated. Always ensure there is a good blood supply to the intestine adjacent to the site of resection to ensure best healing.
Vascular ablation is carried out first by applying ligatures of polyglactin 910 or another absorbable material. This author prefers to use 3m polyglactin in foals and 4m in adult horses and always applies at least two ligatures to each vessel. If more than two metres is to be resected, a long end of suture material is left from one of the pair of ligatures on each major vessel, to permit the ends subsequently to be tied together (Figure 8), ensuring there is minimal risk of creating a “figure of eight” with a twist in the intestine. This complication would require the anastomosis to be repeated. The technique is particularly valuable when greater lengths of intestine are resected.
The use of an electronic vessel-sealing device (LigaSure, from Covidien/Medtronic) can be very useful in more extensive resections (Figure 9), to reduce surgical time. However, in such cases, the author always applies at least one ligature to each arcuate vessel, with a long end to ensure the resected mesentery can be collected together in an orderly manner prior to anastomosis.
Having effectively prevented significant haemorrhage from the mesenteric vessels, a Penrose drain (tied fairly tightly around the intestinal wall and held in place with forceps) can be used aboral to the site of the aboral intestinal section to prevent backflow of ingesta into the peritoneal cavity and its end covered with a sterile large swab to further minimise the leakage of ingesta or bacteria. It is usually safest to apply the drain, passed through a small mesenteric hole, at least 10cm beyond the site to be transected. Another Penrose drain or a pair of Doyen forceps prior to intestinal section should occlude the aboral end of the resected segment.
At this point the mesentery may be transected distal to the ligatures, trying to remove all necrotic mesentery associated with the intestine to be resected. If this is not possible, an attempt should be made to cover any remaining necrotic mesentery with adjacent healthy mesentery, to avoid it becoming adherent to other structures.
The aboral end of the intestinal segment to be resected can be passed to a non-sterile assistant who removes the drain or forceps to allow drainage of the typically distended orad intestine into a bin (Figure 10) or a drain. Gentle massage of the orad intestine facilitates this. This serves two main functions. Firstly, it removes fluid ingesta, which is likely to be full of endotoxins, potentially further contributing to endotoxaemia, and secondly, it empties the intestine, which is an important way of reducing the risk of postoperative ileus. The same procedure of tying a Penrose drain around the intestine is applied orad to the segment to be resected. After resection, its open end (although occluded by the drain) is further prevented from leakage by covering it with a large swab.
The most effective method of anastomosis is “end-to-end”, although other approaches are possible. This offers the most physiological junction and can be rapidly carried out with a one or two-layer hand-sewn technique.
Traditionally, it was thought a jejuno-ileal anastomosis carried a very poor prognosis and it was preferable to use a jejunocaecostsomy “side to side” technique. However, it has been shown the prognosis for “end-to-end” techniques is better and jejuno-ileal anastomoses are preferred to jejunocaecostomy.


Having protected the open ends of the intestine after application of an occlusive Penrose drain and resected the necrotic intestine, the healthy intestinal ends are lined up attempting to join the mesenteric attachment of one side to the mesenteric attachment of the other, although this does not have to be exact.
The author’s preferred technique in the past 30 years is a two-layer approach. Firstly, a continuous appositional mucosal suture of 2 or 3 polyglactin is carried out rapidly to seal the open ends of the intestine (Figure 11) and to act as a template for the more important seromuscular layer. This is carried out with similar suture material using a continuous minimally inverting Lembert suture, interrupted at 180 degrees to avoid creating a “purse-string”.
Once the anastomosis has been performed the Penrose drains are removed. In fact, these can sometimes be removed after the first layer of closure, simply to avoid unnecessary crushing of the intestinal wall. The anastomosis is checked to ensure free passage of ingesta without leakage (Figure 12) and then any remaining mesenteric defects are closed.
When there is no possibility of an “end-to-end” anastomosis (when the distal ileum is involved), the intestine is transected orad to the lesion after vascular ablation, either by the method already described or using a linear cutting staple device – the author uses a 7.5cm gun. In either case, additional closure of the orad intestine is achieved via a Parker-Kerr or similar inverting intestinal suture so a blind end is created.
The intestine is then aligned in a position as near to anatomical normality as possible, between the medial and dorsal caecal bands. Stay sutures can be placed before two stab incisions are created; one is in the ileum or distal jejunum after a Penrose drain has been placed to occlude flow of ingesta; the other is in the caecum, which is elevated and held away from the protected laparotomy incision to minimise leakage, before the staple gun (7.5cm) is assembled with an arm in each lumen (Figure 13) and the gun fired. The gun is then reloaded and turned the other way round before again being fired. In this way a 15cm stoma has been created. The stab incisions are then closed with 3 polyglactin.
To avoid risk of staple pull out (Figure 14), the whole anastomosis is also oversewn with 3m polyglactin in a continuous pattern. Furthermore, to avoid the intestine “kinking” at the anastomotic site, a 10cm section of small intestinal wall orad to it is sutured to the adjacent caecum, to stabilise it and thus avoid obstruction at the stoma. As the site of anastomosis is between the medial and dorsal caecal bands it is usually easy to close any mesenteric defect by incorporating the ileocaecal fold.


A major life-threatening complication of strangulating small intestinal disease can be postoperative endotoxaemia. However, it is not proposed to discuss this complication here, other than to report a number of medical strategies are employed to combat the problem. Various drugs, including aspirin and dalteparin and hyperimmune plasma, have been used to augment routine NSAID medication.

Anastomotic leakage is surprisingly rare following intestinal anastomosis. However, the author has seen anastomotic leakage when staples were used without oversewing the staple line (Figure 15). This suture can be applied very quickly and should be used for all stapled anastomoses to ensure staple security.
Obstruction of the anastomotic site can occur for a variety of reasons. Over-inversion of the seromuscular layer can cause physical obstruction, or at least reduce the flow of ingesta through the anastomosis, creating paralytic ileus. Thus the author always uses a minimally inverting Lembert suture to avoid this complication. This is also the reason for suturing 10cm of jejunum or ileum orad to a stapled “side to side” anastomosis between small intestine and caecum. Thus ingesta does not become obstructed by “kinking” of the small intestine at the anastomosis.
Postoperative haemorrhage is always a risk, particularly in endotoxaemic patients, which may have a clotting problem. This is the reason why robust vascular occlusion is necessary. Some horses examined postmortem after intestinal anastomosis are found to have free blood in the peritoneal cavity, or large blood clots near the site of mesenteric resection. It is worth taking extra time during surgery to ensure vascular ligation is effective.
Postoperative paralytic ileus is common following small intestinal resection. Many horses reflux immediately after surgery, usually because it is not always possible to drain the stomach completely either before or during surgery by routine nasogastric intubation. This reflux is not related to paralytic ileus, which develops typically during the first few postoperative days, when large volumes of gastric fluid are retrieved by nasogastric tube.
Small intestinal distension can usually be identified by rectal palpation or transabdominal ultrasonography. This is the subject for an article on its own, so for this discussion it is only necessary to report that proactive encouragement of intestinal activity using stimulant medication initiated during surgery, restricting postoperative oral intake to a few mouthfuls of grass, appropriate, but not over-zealous, intravenous rehydration, gentle exercise and regular intermittent gastric decompression, are all considered important in reducing the risk of ileus.
A degree of peritonitis almost certainly occurs following every laparotomy, but its severity is typically greater following intestinal anastomosis. Scrupulous intraoperative hygiene and surgical technique will help reduce the risks of this problem and perioperative broad spectrum antibiotics (usually penicillin, gentamycin and, sometimes, metronidazole) are administered routinely.
The development of postoperative adhesions has always been considered to be a major risk following small intestinal resection and probably adhesions develop more frequently than can be assessed clinically. They are of greatest significance when they cause intestinal obstruction or strangulation. Risk factors seem to include peritonitis, ileus and postoperative haemorrhage. Thus avoiding these problems should help reduce the risks of adhesion formation. While most adhesions cause a clinical problem within 12 months of surgery, the author has encountered a case in which 11 years separated surgery and the signs of colic and intestinal strangulation.
While it is usual practice to offer nil by mouth postoperatively, bar a handful of grass periodically, it is easy to neglect the horse’s nutrition. This is particularly so when dealing with pregnant mares. In fact, postoperative support and nutrition can be very important for tissue healing and recovery in all cases. While the best method might involve total parenteral nutrition, this is prohibitively expensive in most cases and may be impractical. However, some form of additional nutrition as 2.5% glucose saline is inexpensive and useful. Monitoring triglycerides using an inexpensive machine is also valuable to assess nutrition status.
In summary, many hospitals are now able to offer colic surgery and the results of small intestinal resection have improved to the point where 75% or 80% survival to hospital discharge are not exceptional these days. However, these are always challenging cases, with many potential complications. A number of these can be minimised by following appropriate technique.