7 Mar 2016
Rebecca Robinson looks at ways in which pain can be assessed in companion animals using the variety of available scales (part 2 of 2).
Celia Marr
Job Title
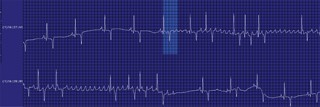
Figure 2a. Post-race ECG recording in a racehorse.
Atrial fibrillation has long been recognised as an important cause of poor performance in horses, but technological advances are providing insights that suggest the problem may be much more common than previously recognised.
Clipless, smartphone-based ECG units are increasingly widely available to equine vets. They are easy to use and high-quality traces can be obtained.
To generate a database of findings in healthy horses, a study is looking at the prevalence of post-race arrhythmias.
We are also much better equipped today to treat atrial fibrillation with either pharmacological or electrical methods. Research on tissue Doppler imaging is proving non-invasive assessment of atrial fibrillation cycle length, together with assessment of left atrial size and post-treatment function, allows clinicians to offer more accurate advice on optimal management and prognosis.
Most equine practitioners recognise atrial fibrillation as a chaotic, irregularly irregular cardiac rhythm they may detect in competition horses, racehorses or hunters with a history of exercise intolerance or poor performance.

It is occasionally picked up during a routine examination, such as a pre-vaccination check, and when this happens the horse is usually not regularly performing vigorous exercise – although they may be competing successfully in dressage, showing or showjumping.
On detecting atrial fibrillation, the next question is whether it is lone atrial fibrillation; is there evidence of underlying, structural cardiac disease? Physical exam findings go a long way towards answering this question.
Clinical signs suggestive of underlying cardiac murmur include resting tachycardia, cardiac murmurs, prominent jugular pulsation, venous distension and peripheral oedema.
Atrial fibrillation is often found in congestive heart failure, but as a consequence and not a cause; the most common underlying pathology is severe valvular disease. Less common causes are congenital cardiac or myocardial diseases (Figure 1).
It has long been recognised some horses with atrial fibrillation will self-correct within 48 hours. This has been best documented when atrial fibrillation is detected after racing, usually disappointingly.
A study performed in Japan between 1988 and 1997 estimated the minimum prevalence of atrial fibrillation was 0.29% (or 1 case in every 341 starts) in horses racing on the flat (Ohmura et al, 2003). More than 90% of cases resolved without treatment within 23 hours.


A more recent survey showed a prevalence of 0.1% in American standardbreds (Slack et al, 2015).
In the UK, a three-year surveillance study (1996 to 1998) conducted into clinical problems during and immediately after racing identified paroxysmal atrial fibrillation at a prevalence of 0.2 per 1,000 starts (Williams et al, 2001).
However, vets who work with racehorses will recognise it is not unusual for horses to come home from racing with a report an arrhythmia was detected after the race, yet no abnormality can be detected the next day, despite extensive investigations.
An ongoing UK project aims to add insight to this dilemma. The post-race ECG project makes use of technology in the hands of many equine practitioners. It is now possible to record an equine ECG using a clipless device attached to a smartphone. This inexpensive device is held over the horse’s chest and sends the trace to the phone via Bluetooth (Figure 2). It takes a little practice, but the device is easy to use (Panel 1) and it is likely it will become commonplace for horse vets to use these devices.
To be able to interpret the clinical significance of any arrhythmia, we need to know what rhythm disturbances are found in horses that have performed to expectations, as well as those showing signs of exercise intolerance.
A team from Rossdales Equine Hospital and the University of Nottingham are performing an ECG survey in horses immediately after racing on six racetracks in the midlands (Figure 2). At the time of writing, just short of 500 ECGs have been recorded and two cases of paroxysmal atrial fibrillation have been identified (Figure 3), suggesting a prevalence of about 0.4% and confirming the suspicion atrial fibrillation occurs more often than previously recognised.

When atrial fibrillation is recognised to be associated with racing or other vigorous exercise, most horses simply need to be allowed to recover and immediate medical therapy is not warranted.
Recording an ambulatory ECG allows the rhythm to be assessed; this can be particularly helpful in identifying more complex rhythm disturbances. Normal sinus rhythm is usually sustained if spontaneously restored. However, in some horses, paroxysmal atrial fibrillation can be a recurrent condition (Figure 4).
Various treatment options are available for horses with sustained atrial fibrillation and no, or minimal, underlying cardiac disease. However, before any therapy, it is prudent to consider if treatment is necessary.
The horse’s current exercise level is an important consideration. With retired horses, or those kept for breeding, their clinical status and general health is often unaffected by atrial fibrillation.
There is no data to help clinicians answer the question often at the forefront of the minds of owners of riding horses diagnosed with atrial fibrillation: is my horse safe to ride? Clinical experience suggests many horses can cope very well with low-level exercise. However, there are anecdotes of horses collapsing and dying once this diagnosis has been made.
The important point to appreciate is not all cases are identical; more complex rhythm disturbances may be present.



A consensus statement from the American College of Veterinary Internal Medicine and the European College of Equine Internal Medicine, on the management of equine athletes with cardiovascular abnormalities (Reef et al, 2014), recommended: “Because safety is a concern with persistent atrial fibrillation, the horse should be cardioverted or retired when the exercising heart rate during sustained maximal exercise exceeds 220bpm, or if concurrent ventricular arrhythmias are detected during exercise or with sympathetic nervous system stimulation.”
It also stated: “Horses with persistent atrial fibrillation should only be ridden or driven by an informed adult and limited to an exercise level considered relatively safe based on an exercising ECG. The use of a heart rate monitor might be useful to track heart rate during exercise and modify the rigour of the work performed.”
Two modes of therapy for rhythm correction are well established in horses – pharmacological conversion and electrocardioversion. Both have potentially harmful effects and selection of the most appropriate therapy is primarily based on predicted efficacy for the specific case.
Unfortunately, there has been no randomised controlled trial comparing the two approaches – and differences between patient populations make direct comparisons between studies problematic.
Quinidine sulphate has been used to treat atrial fibrillation for more than 50 years. It is generally given by nasogastric tube at two-hour intervals for four or five treatments, then the dosage interval is extended to six hours to try to achieve fairly steady plasma concentrations until either sinus rhythm is restored or side effects force the treatment to be stopped.
The prognosis for horses with minimal heart disease is fairly good, provided the duration of the atrial fibrillation is fairly short (about one month), but side effects become more common in horses that have had atrial fibrillation for some time (Reef et al, 1988).

Transvenous electrical cardioversion (TVEC) is often preferred for horses that have atrial fibrillation of unknown or known, prolonged duration. These horses typically perform less vigorous exercise where the dysrhythmia has gone unnoticed.
TVEC was initially described in standardbreds with short duration atrial fibrillation and very high rates of conversion were achieved (McGurrin et al, 2008). The technique involves placing electrodes in the left pulmonary artery and the right atrium, with guidance from a combination of pressure profiles, ultrasonography and radiography (Figure 6). This is performed under standing sedation; general anaesthesia is induced and incremental biphasic electrical shocks are given.
Sustained atrial fibrillation leads to electrical, mechanical and contractile remodelling in the atrial myocardium.
In humans, tissue Doppler imaging methods of assessing left atrial electromechanical conduction time is a useful prognostic predictor. Research in sustained atrial fibrillation in horses has focused on improved methods of assessing atrial dimensions and function that, in turn, may help refine more appropriate post-treatment management and provide additional prognostic information.

Evidence shows the ratio of the atrial fibrillation cycle length to the left atrial size (corrected to the size of the aorta) is a useful predictor of recurrence (De Clercq et al, 2014). In this study, atrial fibrillation cycle length was measured with intra-atrial ECG; however, this can also be accurately estimated non-invasively with tissue Doppler imaging (Figure 7; Decloedt et al, 2014).
A large multi-centre study on atrial fibrillation recurrence has shown a rate of 39% at one year in horses treated for the first time. A history of previous atrial fibrillation and low left atrial fractional area change were significant predictors of recurrence (Decloedt et al, 2015).
Together, these studies provide exciting evidence: using advanced ECG imaging techniques can now help clinicians predict recurrence of atrial fibrillation with more accuracy than previously possible.