21 Aug 2023

Image: © kobkik / Adobe Stock
Canine atopic dermatitis (cAD) is a common hypersensitivity skin disease in dogs for which treatment can, on occasion, be complicated.
Before starting therapy, owners should be made aware that cAD is an incurable disease requiring chronic therapy. Treatments fall into the following categories – each addressing different aspects of the pathogenesis of cAD:
The aim of therapy is to keep the patient lesion and pruritus free, while using the lowest dose and frequency of medications. Using multimodal therapy, clinicians are often able to reduce the dose of individual treatments, minimising adverse effects.
cAD presents with variable degrees of pruritus and inflammation. The combination and relative severity of these signs should underpin clinicians’ decisions when choosing medical therapy. A client’s ability to apply treatments and financial constraints also must be considered.
ASIT is the only treatment that addresses the underlying disease mechanism in cAD. It is formulated based on the results of intradermal testing and/or allergen-specific serum IgE testing. The clinician must have local knowledge of potential allergen exposure, seasonality and the dog’s history to design a suitable prescription. Immunotherapy uses gradually increasing doses of allergens to induce tolerance against the offending allergens.
It is reported that in 50% to 80% of patients receiving ASIT there is at least a 50% reduction in clinical signs and medication requirement.
The time it takes ASIT to become effective can vary and, in some individuals, may be up to 8 to 12 months. This should be discussed with owners to prevent premature cessation of the treatment due to perceived lack of efficacy.
The patient should also be started on additional maintenance therapy during the initial course of ASIT, such as those discussed later, to maintain patient comfort. This maintenance therapy should be periodically (every few months) withdrawn or tapered to assess the response to ASIT.
ASIT appears to be safe to use in the long term; however, occasional reactions can occur after administration (especially in the induction phase). The most concerning side effect is anaphylaxis, which is fortunately very rare and is less likely with European alum-precipitated products. For this reason, it is advised that the first five to six injections are performed at the veterinary practice before owners potentially learn to administer the medication at home.
Occasionally, a slight increase in pruritus can be seen after administration. In these cases a dose reduction and more gradual introduction of the ASIT should be considered.
Flare factors exacerbate a patient’s atopic dermatitis. Common canine flare factors include flea bite hypersensitivity, other parasitic infestations, secondary microbial overgrowth/infection and food or environmental allergen exposure.
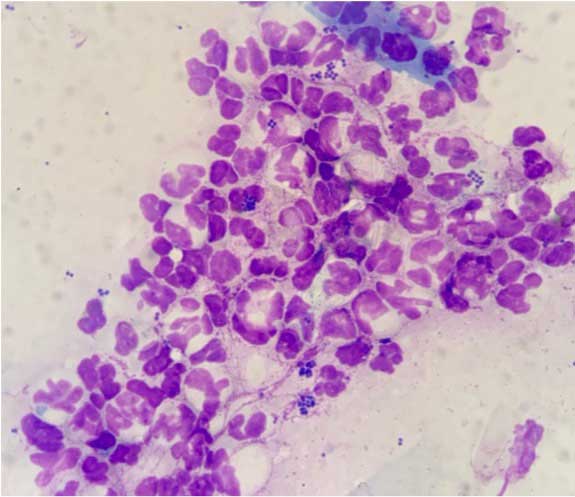
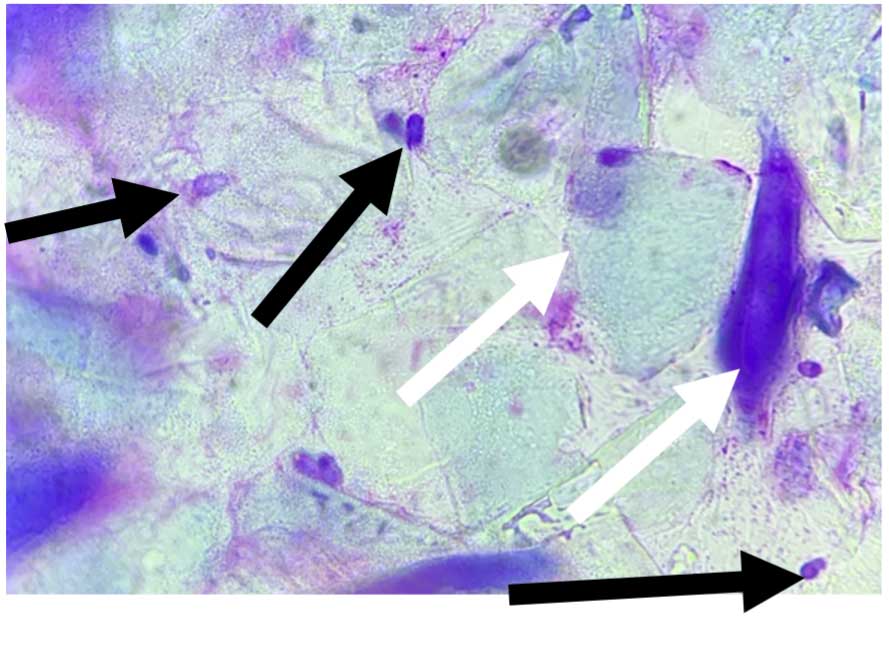
Newly diagnosed and previously stable patients suffering from a cAD flare should have cytology performed on lesions to assess for inflammation and microbial overgrowth/infections (Figures 1 and 2).
Topical therapy should be considered as first line treatment for antimicrobial stewardship. Chlorhexidine or dilute hypochlorous acid are usually effective. The former is available as sprays, wipes, foams or shampoos. The choice of product can be tailored to owner and patient preferences to enhance compliance.
When using these products during a flare, frequent application is required – for example, twice-weekly bathing for two weeks in a 2% to 4% chlorhexidine shampoo, with daily use of an antiseptic impregnated wipe between baths. After lesion resolution, a reduction – but not cessation – of therapy may help to prevent future flares. Regular flares of bacterial or yeast (for example, Malassezia pachydermatis) overgrowths often may indicate inadequate control of the primary pruritus and inflammation.
Corticosteroids are commonly used in cases of cAD to control both pruritus and inflammation. They have a rapid onset of action, doses can be tailored to the individual patient, they are inexpensive and they are generally easy to administer.
When patients present with an acute flare of disease (pruritus or inflammation) a short course of prednisolone (for example, 0.5mg/kg total daily dose for three to five days for in mild to moderate cases) will generally settle the clinical signs. This may be required at the beginning of the pollen season, or when the patient is exposed to another flare factor – for example, dietary indiscretion.
The use of steroids to control allergic flares are low risk if only required a few times a year. In cases where there are chronic changes to the skin, such as lichenification and hyperpigmentation, longer courses or higher doses will be required for lesion resolution. There is no evidence to suggest that a patient’s total dose of prednisolone split into twice-daily dosing has different clinical effects to once-daily dosing. Once-daily dosing may lead to better owner compliance.
In the short term, the most common adverse effects are polyphagia, polydipsia, polyuria, vomiting and diarrhoea. If these signs are excessive or problematic in an individual, a change to methylprednisolone can be tried.
Methylprednisolone is 1.2 times as potent as prednisolone. Practically, a 4mg methylprednisolone tablet is the equivalent of a 5mg prednisolone tablet. Recent work by Lokianskiene et al (2022), has shown that clinically there may be no difference between these glucocorticoids when comparing daily water intake and urine specific gravity.
For all of the benefits of glucocorticoid therapy, long-term effects exist (Panel 1). Their use for chronic treatment of cAD should be reserved for cases with great financial constraints or that are refractory to other treatments. In these cases, the lowest effective dose and frequency of administration required to control the clinical signs should be sought.
Every other day dosing of glucocorticoids can help to reduce the clinical signs associated with longer-term therapy, while keeping the patient pruritus and lesion free.


Two veterinary-licensed topical steroid sprays are available – hydrocortisone aceponate and triamcinolone acetonide – that have been shown to be beneficial in a number of diseases, including cAD.
An advantage of topical corticosteroids is they can be applied exclusively to the affected area – for example, interdigital spaces or ear pinnae.
As with systemic steroids, skin thinning can be seen with these topical products. One product – hydrocortisone aceponate – is a di-ester topical glucocorticoid. This is metabolised in the skin to largely inactive moieties that help to avoid localised side effects.
A dose of one pump per 5cm2 is advised by the drug manufacturer. Good results are often seen with daily application for 7 to 14 days, successfully reducing the signs of mild-moderate pruritus and inflammation. At this stage, an off-licence reduction to twice to three times weekly application appears to be adequate for maintenance control.
Care should still be taken and regular veterinary assessments undertaken during maintenance treatment, as overuse, or frequent use in an area of thin skin (axillae/abdomen), can lead to skin thinning, milia, comedones and alopecia.
Ciclosporin is a good anti-inflammatory therapy with moderate anti-pruritic activity. It is an ideal treatment for the long-term control of cases with a large inflammatory component of their disease. These often present clinically with erythema, lichenification and seborrhoea.
In cases with pododermatitis leading to pedal folliculitis and furunculosis (interdigital cysts) ciclosporin is often the long-term treatment of choice to reduce the inflammation driving foreign body reactions to keratin from follicle rupture.
Ciclosporin is a calcineurin inhibitor that downregulates the synthesis of numerous pro-inflammatory cytokines including IL-2 and interferon g. The dose is 5mg/kg every 24 hours.
Ciclosporin has a slow onset of action as it can take four to six weeks for full efficacy. A course of glucocorticoids – dosed as above – during the induction phase has been shown to decrease the time to maximal clinical effect, with the added benefit of keeping the patient comfortable during this time.
In some cases, once good clinical control has been reached, the frequency of administration may be reduced to every two to three days. Gradual alterations in treatment should be performed with frequent examinations to check the response. Although the initial cost of daily ciclosporin is high, if reduced frequency/dosage is achieved, longer-term financial outlays are often comparable to other medications – for example, oclacitinib.
Anorexia, diarrhoea and vomiting can occur when ciclosporin is started. To reduce the incidence of side effects, a gradual introduction of the medication over around seven days can be useful.
Contrary to the data sheet, giving the medication with food is unlikely to affect the overall clinical outcome of the medication, and may reduce adverse gastrointestinal effects. For example, an induction dose for a 30kg dog would be 50mg once daily for three days, then 100mg once daily for three days, then 150mg once daily ongoing.
Liquid formulations (100mg/ml) are also available, which may be useful in patients that are difficult to tablet and allows more flexibility with dosing. Longer-term, adverse effects can include gingival hyperplasia and hirsutism.
In some cases of gingival hyperplasia, dose reduction (if possible) or surgical resection – for example, with a CO2 laser – may be necessary. The data sheet states that ciclosporin is not used in cases with a history of malignant disorders or progressive malignant disorders.
Oclacitinib is a useful treatment option in pruritic atopic cases. Oclacitinib is a preferential JAK-1 selective inhibitor. At doses above the licensed protocol it may inhibit the JAK-2 pathway that is involved in haematopoiesis. A reduction in pruritus and inflammation occurs by the inhibition of the JAK-1 pathway and reduction of the following cytokines: IL-2, IL-4, IL-6, and IL-13 and IL-31.
Oclacitinib has a fast onset of action and is often effective within 3 hours of administration (Fleck et al, 2022). The dosage is 0.4mg to 0.6mg every 12 hours for 14 days, before a reduction to 0.4mg/kg to 0.6mg/kg every 24 hours. It does, however, have a short half-life of 4 hours and so in some cases may not be clinically effective for a full 24-hour period. Therefore, the time of dosing can alter the overall effect of treatment.
If the patient is more pruritic in the evening when relaxing at home, but is busy and distracted in the morning, dosing in the evening can be considered. Oclacitinib appears less effective against moderate to severe otitis and hyperplastic pododermatitis, and so other therapies may be required in these areas (for example, topical and systemic glucocorticoids).
Periodic monitoring, haematology and biochemistry is advised by the manufacturer when patients are on long-term therapy. This is due to the potential effects on haematopoiesis, although during clinical trials changes were mild and within the reference range.
The authors have occasionally encountered mild hypercholesterolaemia and neutropenia that has corrected on reduction of oclacitinib dose in the clinical setting. The exact frequency of blood tests is at clinicians’ discretion, but the authors often perform them every 6 to 12 months. Side effects include a low incidence of vomiting and diarrhoea (1 to 10% of dogs treated).
As per the data sheet, this product should not be used in patients under 12 months old. As oclacitinib is an immunomodulator, the data sheet also states it may increase susceptibility to infection and exacerbate neoplastic conditions. Therefore, it should not be used in the face of severe infections or when a patient has a malignant tumour.
Lokivetmab is the most recently licensed anti-pruritic treatment. Lokivetmab is a caninised monoclonal IL-31 antibody (a known pruritogen in dogs). Due to its action on IL-31, lokivetmab is useful in patients with pruritus.
In cases of moderately severe inflammation the authors will often initially control symptoms with a broader-spectrum anti-inflammatory – for example, glucocorticoids. Once the acute flare has been managed, if the first sign of disease relapse is pruritus, lokivetmab can often be used to good effect to prevent further flares of disease in the longer term.
The UK licensed dose is 1mg/kg SC every four weeks. The manufacturer guidelines state that two doses should be given before final judgement of efficacy is taken. In some cases, a limited response may be seen after the first dose. In such cases a greater response may be observed after a second dose. If there is no improvement after two months, lokivetmab is not suitable for the patient.
In some cases, it may be possible to increase the dosing interval once patients have been stable on lokivetmab for several months. In cases with significant and particularly chronic inflammation – such as recurrent otitis and hyperplastic pododermatitis – lokivetmab is not suitable for sole therapy.
The role of antihistamines in the control of cAD is limited and little evidence exists for their use (DeBoer and Griffin, 2001). The absorption, metabolism and response can vary between formulations, and in individual patients. Their use as first line therapy in cAD is not advised. Side effects include sedation and it is possible this will be perceived as a reduction in pruritus by the owner.
The outermost layer of the skin (stratum corneum) is made up of corneocytes and lipids, and is disrupted in cAD. The function of this layer is to reduce water loss from the skin and reduce pathogen and allergen entry. Reduction in barrier function induces cutaneous inflammation and contributes to the clinical signs.
Topical moisturisation is a mainstay of treatment in human atopic dermatitis, and this treatment can also be used in dogs. Products containing propylene glycol act as a humectant (increasing the water binding capacity of the stratum corneum). The use after bathing has been shown to reduce transepidermal water loss (Panzuti et al, 2020).
In models of chronic skin barrier disruption, propylene glycol has also been shown to increase the thickness of the stratum corneum and reduce the dermal inflammatory infiltrate. Although unlikely to entirely control cAD alone, as part of a multimodal treatment regime, its use may reduce the overall treatment burden.
Dietary polyunsaturated essential fatty acids (PUFAs) can also be used to improve the skin barrier. They affect the water-holding ability of the stratum corneum and control of epidermal proliferation and differentiation.
Dogs fed diets formulated with increased levels of PUFAs can have a reduction in their overall level of pruritus and lesion scores. For example, one complete diet contains a novel HistaGuard complex designed to reduce histamine and pro-inflammatory cytokine release on the patient’s exposure to environmental allergens. The diet contains egg as whole protein – a rare allergen in dogs seen in only 4% of those with food allergy (Mueller et al, 2016). Complete diets like these can be an easy adjunctive treatment for owners.
Some owners will consider supplementing their pets’ current diet with essential fatty acids, which are available as liquid or capsule preparations.
Occasionally, a previously well-controlled patient will present with increased pruritus, despite following a treatment plan. In these cases clinicians can often find a logical underlying reason. The general health of the patient, comorbidities and the treatment regime should be assessed.
Investigations into exposure to flare factors – for example, flea bites or microbial overgrowth – can often be rectified easily with either a return to ectoparasite control or increased topical antimicrobial therapy. In some cases, other pruritogenic diseases should also be considered – for example, scabies or epitheliotropic lymphoma in older dogs.