13 Jan 2025
The World Health Organization (WHO, 2023a; 2023b) identifies climate change as the foremost threat to humanity, exacerbating crises such as heatwaves, wildfires, floods and storms, affecting 3.6 billion people.
By 2030 to 2050, it could lead to 250,000 additional deaths yearly due to undernutrition, malaria, diarrhoea and heat stress. Urgent action is imperative to mitigate risks and enhance public health.
In the UK, health care is a major energy consumer, with the NHS contributing 25% of emissions in the public sector. Surgery theatres within hospitals are particularly resource intensive. Implementing emission reduction strategies in these areas is expected to yield significant benefits (MacNeill et al, 2017). Similar findings can be expected in the veterinary sector.
The NHS has committed to net zero by 2045, with an ambition to reach an 80% reduction by 2036-39 (NHS, 2022).
With these considerations, Willows Veterinary Centre and Referral Specialists made a decisive commitment during last summer’s environment committee meeting to prioritise reducing the carbon footprint of surgical procedures in the forthcoming months.
To comprehensively address this objective, two identical surgeries were conducted, both being brachycephalic obstructive airway syndrome (BOAS) procedures.
However, one surgery incorporated every feasible measure to minimise carbon emissions, while the other followed conventional protocols.
Subsequently, the carbon outputs of each procedure were compared, aiming to identify effective strategies that could be universally implemented across all surgeries to mitigate environmental impact.
In efforts to significantly diminish the environmental impact of surgical procedures, the following areas were meticulously examined by the surgical team at Willows:
The surgical team for the carbon surgery all opted for carbon-neutral commuting by cycling to work that day. Recognising the significant role of cars in greenhouse gas emissions, with the combined mileage for the routine surgery totalling 151 miles, this was a substantial reduction in CO2 emissions.
While achieving commuting to work in a carbon-neutral manner may not be feasible for everyone, promoting initiatives such as the cycle to work scheme can benefit practices. Advertising these schemes to staff not only contributes to environmental sustainability, but also offers significant physical and mental health benefits to staff (Department for Transport, 2019).

Before commencing the reduced carbon surgery, a thorough analysis was conducted on all surgical items to determine their necessity for the procedure. This involved examining specific surgical kits, such as the BOAS kit, to ensure only essential items were needed to reduce sterilisation.
By utilising surgical metal tins to organise kits, the need for multiple autoclave cycles and individually pouched items is minimised. These kits are designed to contain everything necessary for performing a surgery. As a result of this process, certain items were added, leading to a 50% reduction in the usual number of pouched items in the operating theatre.
Rigid container systems come in aluminium, stainless steel, plastic or a mix. They are equipped with lid filters for sterilisation and keeping out microorganisms, ensuring items remain sterile.
Depending on the container maker, filters can be reused or thrown away. Inside is often a basket with handles for holding instruments, making them easy to move around in a sterile way. But they can have a higher upfront price and can be heavy to lift. Also, the bigger containers will not fit into small autoclaves and will take up more space than pouches; however, smaller containers are available.
Maintenance, such as cleaning and checking for damage, is crucial, too (Caveney, 2011). Nevertheless, as lots of surgical equipment is commonly packaged in disposable sterilisable packets composed of paper and a composite plastic, this offers an eco-friendlier alternative for veterinary practices.
In response to escalating concerns about surgical site infections (SSIs), operating theatres are increasingly transitioning to reusable items, driven by a burdening environmental consciousness.
This transition, a key focus for the environmental committee, was thoroughly examined for this surgery. Among the most straightforward items of personal protective equipment to adapt are surgical hats. Recent studies have debunked any link between the type of surgical hat worn and SSI risk.
Remarkably, the University of Amsterdam (2023) posited that substituting 10 million reusable caps for 1 billion disposable caps globally could potentially curb CO2 emissions equivalent to the yearly output of 2,000 passenger cars.
An alternative strategy to mitigate environmental impact involves embracing reusable surgical gowns and drapes. Research by Vozzola et al (2020) illuminated significant reductions across multiple environmental metrics when opting for reusable gowns. With advancements in reusable fabric technology and improved risk reduction measures, the use of reusable gowns for procedures with lower fluid levels is becoming increasingly prevalent. Our investigation also delved into the use of drapes, ubiquitous in veterinary practice and available in both reusable and disposable variants. These drapes play a pivotal role in curbing external contamination and averting contamination transfer to the surgical site.
Despite some ambiguity in recommendations, findings from Vasanthakumar (2019) yielded mixed results, with the disposable drape group showing promise in reducing SSI risk and air bacterial counts. However, uncertainties persist due to study limitations.
Nevertheless, for low-risk surgeries such as elective clean procedures, veterinarians may contemplate adopting reusable drapes to minimise waste without compromising patient well-being.
One focus of reduced carbon surgery was to minimise waste and ensure proper waste management.
Information on waste generation in veterinary practice is limited, unlike the human medical field where operating theatres significantly contribute to hospital waste. During both the surgeries, all waste underwent meticulous weighing and sorting for appropriate disposal.
Although much medical waste is deemed to be no more dangerous than household waste, approximately 35% consists of plastic materials, providing opportunities for recycling and sustainable resource recovery. Therefore, prioritising recycling and correct waste disposal practices is essential (Singh et al, 2022).
Medical waste includes various types, such as infectious waste, requiring specialised handling. Traditional disposal methods, such as incineration, have caused air pollution. However, waste reduction can begin immediately through the principles of reduce, reuse and recycle. Hospitals have effectively managed waste by forming collaborative stewardship teams and raising awareness of ecological impacts.
In veterinary practices, understanding waste output and implementing reduction strategies is crucial (Vasanthakumar, 2019). Proper waste segregation reduces environmental pollution and manages costs effectively, as hazardous waste contains harmful substances that can contaminate soil, water and air (WHO, 2018), and non-hazardous waste is cheaper to dispose of (United Nations Environment Programme, 2015).
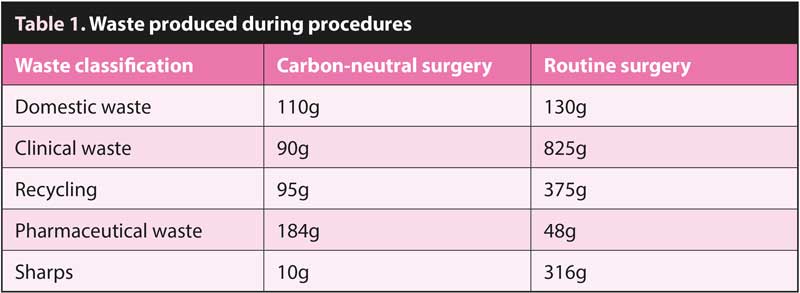
To effectively monitor and reduce waste in our reduced carbon surgery, we implemented stringent measures to minimise waste generation. To quantify the impact of these measures, we weighed all the waste produced during the procedure, as detailed in Table 1. These efforts resulted in a significant reduction, with the waste generated amounting to only 29% of that produced in the standard surgical setting.
It has been suggested that halogenated agents (such as isoflurane or sevoflurane) and nitrous oxide (N2O) used to anaesthetise humans contribute to 5% of the carbon footprint of NHS acute care trusts (Narayanan et al, 2022).
When these halogenated anaesthetic agents enter the atmosphere, they obstruct infrared radiation from escaping into space and, therefore, cause retention of heat within the earth’s atmosphere (Andersen et al, 2012).
For both cases presented in this paper, the premedication consisted of intramuscular medetomidine and methadone. After pre-oxygenation, anaesthesia was induced with propofol given intravenously to effect via a pre-placed IV cannula, orotracheal intubation was performed and 100% oxygen supplied via a circle rebreathing system.

For the reduced carbon case, TIVA with propofol, fentanyl and medetomidine infusions were started with the use of syringe drivers to maintain anaesthesia. For the conventional case, isoflurane vaporised in oxygen was used. Electrical supply for equipment was considered carbon neutral, as the hospital’s energy supplier provides 100% renewable energy.
While performing anaesthesia without volatile anaesthetic agents will reduce carbon emissions, the emissions caused by the increased number of syringes associated with a TIVA technique should be considered. In a study comparing inhalational anaesthesia and TIVA techniques, Greaves and Fletcher (2020) showed that, despite increasing single-use items and drugs associated with TIVA, an overall reduction in kgCO2e still occurred with this technique compared to anaesthesia maintained with sevoflurane (7.97kgCO2e and 10.72kgCO2e, respectively).
The production and disposal of single-use plastics, such as syringes, may have negative impact on the environment, with 1kg of polyvinyl chloride producing 6kgCO2e over its lifetime (Greaves and Fletcher, 2020). While the use of disposable items is usually unavoidable in health care due to patient safety and sterility concerns, the source can be selected by the user to ensure environmental impacts are minimised.
The syringes used for the presented case were from a factory, of which their manufacturing process uses 100% renewable energy and of which distance from the UK is shorter compared to other manufacturers, reducing emissions related to transportation (BD, 2024).
Another consideration to take into account when using TIVA is the effect of the drugs and their metabolites used on contamination of waste water, and their effect on aquatic life. In humans, propofol and its metabolites have been detected for more than 60 hours in urine (Bleeker et al, 2008). These products will eventually be found in waste water.
A review by Waspe and Orr (2023) concluded that current exposure concentrations of these products in waste water were less than the values that would affect aquatic life. In our case, we need to consider that veterinary patients urinate directly on the soil; therefore, the concentrations of propofol and its metabolite (or of any IV drug used which is eliminated from the kidney) will differ from the human model. More recently, techniques to prevent volatile agents from entering the atmosphere have been discussed (Linnaeus, 2024). Volatile capture technology aims to absorb the agent via the scavenging rather than being vented to the environment.
These absorbed agents can be collected and potentially “recycled” by being extracted and reprocessed, which can be reused by hospitals, thereby reducing manufacture of volatile agents and reducing their release into the atmosphere (Gandhi et al, 2024).
While not commonly used in practices at present, their future use has the potential to substantially reduce the escape of halogenated agents used in veterinary practice.
Once again, the carbon footprint associated with the process of capturing these gases needs to be taken into consideration (Sherman and Chesebro, 2022), but the likelihood is that the total carbon footprint will be massively reduced.
Conducting the reduced carbon surgery demonstrated the potential for significantly lowering the carbon footprint of surgical procedures through targeted strategies.
A comparison of the two surgeries revealed a 97% reduction in carbon output for the minimised carbon surgery.
Key actions included carbon-neutral commuting, reducing the use of sterilised items, opting for reusable materials, managing waste efficiently, and transitioning to TIVA.
While not all measures are practical for every surgery, the study at Willows Veterinary Centre emphasises that small changes can significantly reduce emissions.
This encourages the wider adoption of sustainable practices to combat climate change and improve public health.