9 Nov 2021

Image © Ermolaev Alexandr / Adobe Stock
Thoracolumbar intervertebral disc extrusion is a common reason for presentation in clinical practice, most commonly occurring in the miniature dachshund.
Despite extensive research significant unknowns remain, making a balanced and informed comparison between conservative and surgical management challenging.
This article will use a case to highlight the questions that remain and how the authors’ prospective study aims to begin to answer them.

A 4‑year, 10‑month‑old female neutered miniature dachshund presented following a one‑week history of back pain, which progressed over the first 24 hours to paraplegia with an absence of deep pain sensation (reported by a European College of Veterinary Neurology‑registered specialist in neurology).
Due to financial constraints, she was enrolled into our study, having, four months prior to presentation, undergone a left‑sided hemilaminectomy for treatment of an L2-3 intervertebral disc extrusion (IVDE) at a different referral hospital, from which she was reported to have made a full recovery.
On presentation, her general physical examination was normal, with increased body condition score (BCS 7/9) and weighing 5.8kg.
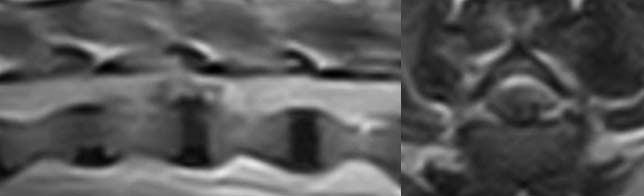
Her neurological examination on arrival at the University of Cambridge Queen’s Veterinary School Hospital revealed paraplegia with intact deep pain sensation. An MRI was performed under sedation with medetomidine 5ug/kg and methadone 0.2mg/kg IM, and demonstrated a severely compressive T13-L1 IVDE (Figure 1).
Thoracolumbar IVDE is a common reason for presentation in clinical practice (Brisson, 2010; Parent, 2010).
It can occur in any breed, but most commonly occurs in chondrodystrophic breeds such as the miniature dachshund (Brisson, 2010). In fact, a recent study showed IVDE has a lifetime prevalence of 20% in the miniature dachshund and will be fatal in a quarter of those (Bergknut et al, 2012).
The signs of IVDE range from back pain alone to paraplegia with loss of deep pain sensation and potentially progressive ascending‑descending myelomalacia (Brisson, 2010). These signs are caused by the herniation of degenerate nucleus pulposus through a ruptured annulus fibrosus, resulting in both a contusive injury to the spinal cord and persistent compression (Brisson, 2010).
The volume of extruded material found on cross‑sectional imaging and at surgery, and the time period over which the material extrudes, varies greatly – meaning each extrusion is a unique combination and interaction of these two insults.
A general perception exists that the most severely affected dogs require surgical decompression – and it seems logical that where compression of the spinal cord is seen, the compression should be removed. This seems all the more reasonable when considering that extensive research has failed to develop a treatment that specifically targets the contusive injury (Vale et al, 1997; Jeffery et al, 2016).
In vitro, it has also been shown that a contused spinal cord is less able to withstand compression than a healthy one (Dimar et al, 1999; Shields et al, 2005), and that chronic mild compression can cause a reversible block of conduction and disruption of myelin and potassium channels (Shi and Blight, 1996; Ouyang et al, 2010).
Furthermore, long-term dynamic compression has been shown to damage both grey and white matter (Wright and Palmer, 1969; Harkey et al, 1995), and residual compression after surgery has been linked to delayed recovery following disc extrusion (Forterre et al, 2010; Hettlich et al, 2012).
While this is a convincing argument for surgery, many unknowns still exist. Dogs with severely compressive thoracolumbar disc extrusions have been reported to have relatively mild symptoms (back pain only; Sukhiani et al, 1996), while other non‑ambulatory dogs have been shown to have comparatively mild compressions (Besalti et al, 2005; Penning et al, 2006).
No correlation exists between the degree of compression seen on MRI and the severity of clinical signs or prognosis (Besalti et al, 2005; Penning et al, 2006).
Furthermore, both canine and human studies have documented the removal of extruded material over time by phagocytosis (Prata, 1981; Hong and Ball, 2016). In one such case, a 69% reduction occurred in just five weeks (Steffen et al, 2014).
Several studies have demonstrated residual disc material left after decompressive surgery having no adverse impact on outcome (Roach et al, 2012; Huska et al, 2014). It has also been demonstrated that a majority of dogs will recover unassisted ambulation when managed conservatively; estimated to be 50% to 100% in dogs that retain deep pain sensation (86% overall; Levine et al, 2007; Joaquim et al, 2010; Freeman and Jeffery, 2017; Langerhuus and Miles, 2017).
This figure is subject to significant bias, with a greater proportion of less severely affected dogs being included in most studies, but still gives credence to the idea that decompression is not always necessary for recovery.

The prognosis for conservatively managed deep pain‑negative dogs is reported to be much lower (6%), although this is based on a very small number of cases so should be interpreted with significant caution (Freeman and Jeffery, 2017; Langerhuus and Miles, 2017).
Interestingly, the prognosis for all dogs – including those that do not retain deep pain sensation – is very similar when comparing fenestration as a treatment for IVDE with decompressive surgery, adding to the evidence that decompression is not the sole answer to the problem (Freeman and Jeffery, 2017).
The combination of this evidence suggests that decompression is not always required for clinical recovery and persistent compression will not alter the prognosis for many cases.
The comparatively limited evidence for conservative management – and strong evidence to support success following surgical management (but not its necessity for clinical recovery) – make it very difficult for veterinary surgeons to recommend conservative management, especially in the most severely affected dogs.
This, combined with the high financial costs of cross‑sectional imaging and surgery, mean a significant number of dogs may be being euthanised when they could have recovered with medical management and some are potentially undergoing surgery when they could have been recovered medically.
No randomised clinical trials are taking place to compare surgical and conservative management of IVDEs. While this would likely be the quickest route to untangling the conflicting evidence, a lack of clinical equipoise means such trials would be very difficult to run.
It does, however, mean many questions remain unanswered. At the Queen’s Veterinary School Hospital, we are recruiting for prospective studies that aim to answer some of these questions.
We are recruiting dogs that are less than 15kg and are non-ambulatory as a result of a suspected thoracolumbar IVDE, and whose owners are unable to afford surgical management.
These dogs will initially receive a subsidised consultation and MRI under sedation to confirm the diagnosis of an IVDE. We will then assist them through 12 weeks of conservative management, at the end of which they will receive another consultation and MRI.
Throughout the 12 weeks, regular contact will occur with the neurology team – allowing us to monitor and manage any complications, and ensure welfare is not compromised.
To this end, we will also ensure all owners are comfortable with bladder management and its potential complications, monitoring for pressure sores and the signs of ascending-descending myelomalacia, as well as liaising with primary care practices. This will allow us to:
The patient was managed conservatively with a short course of meloxicam 0.05mg/kg once daily and gabapentin 17.2mg/kg twice daily, and strict cage rest for four weeks. She also received physiotherapy at home – including massage, passive range of motion and assisted standing exercises – with support from the Queen’s Veterinary School Hospital.
To ensure no evidence existed of persistent back pain, she was presented to her primary care practice shortly after discontinuing analgesic medications for assessment using the Glasgow Composite Pain Score.
The owner reported a return to ambulation (at least 10 steps unaided) 23 days after her initial signs. On follow-up 12 weeks after the initial MRI she was ambulatory paraparetic, with a mild proprioceptive ataxia. Proprioception was normal in all four limbs and all spinal reflexes were normal. Some mild pain on palpation of the mid-lumbar spine was noted.
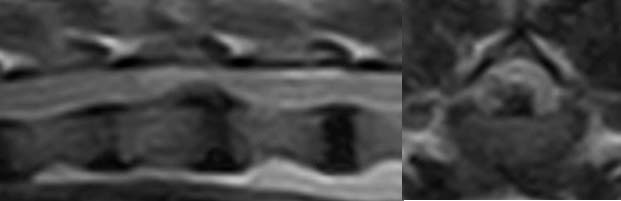
An MRI demonstrated very minimal change in the degree of compression (Figure 2), but the disc material had become more uniformly hypointense on T2‑weighted images.
This case clearly does not prove anything, but it does demonstrate that even the most severely affected dogs have the potential to recover following thoracolumbar extrusions given time and appropriate conservative therapy; visualising a severe compression on MRI does not mean decompression is essential for recovery in all dogs.
To date we have enlisted 19 dogs, of which 16 have recovered ambulation – including 4 out of 6 dogs that were grade five at presentation.
We still have much to learn about conservative management of IVDEs, and it is our hope that this study will move us closer to answering some of these questions.