12 Apr 2023
Q fever – a zoonotic disease with underestimated consequences
This article draws attention to Q fever, which is a cause of reproductive diseases in cattle and small ruminants. It is a zoonosis, yet sorely lacks the necessary national recognition to successfully eradicate it.
Jonathan Statham
Job Title
Figure 6. Recent calving with placental tissue and calf with cow.
Q fever is a zoonotic disease caused by Coxiella burnetii, a bacterium which is found worldwide in a range of animals.
Infection may cause abortions, infertility, metritis or chronic mastitis, which can lead to economic losses for infected herds. Since 2007, Q fever has been emerging as a public health problem in several parts of Europe, as well as further afield. Although asymptomatic in 60% of human cases, it can lead to acute or chronic infections and cause flu-like syndrome, hepatitis, pneumonia, endocarditis or abortions.
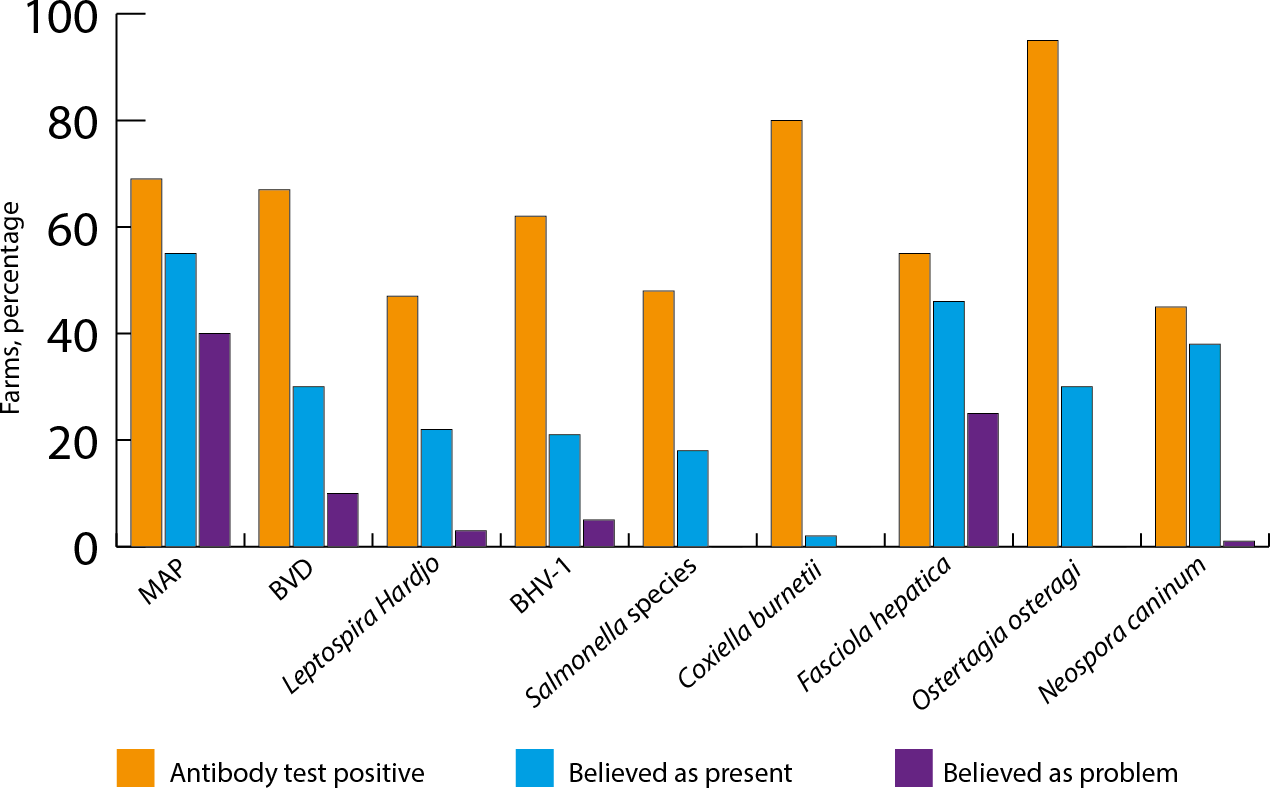
Q fever has underestimated consequences in UK herds. It is a disease with low levels of recognition. Although its impact should not be taken out of the context of high impact diseases – such as bovine viral diarrhoea (BVD), infectious bovine rhinotracheitis (IBR), Johne’s disease and bTB – the gap between recorded prevalence and perception is wide.
Velasova et al (2017) reviewed herd level prevalence of selected endemic infectious diseases of dairy cows in Great Britain. Although approaching 80% of surveyed herds were C burnetii seropositive, only 1% to 2% of farmers believed the disease was present on their farm, and 0% perceived the disease was a problem (Figure 1).
Aetiology
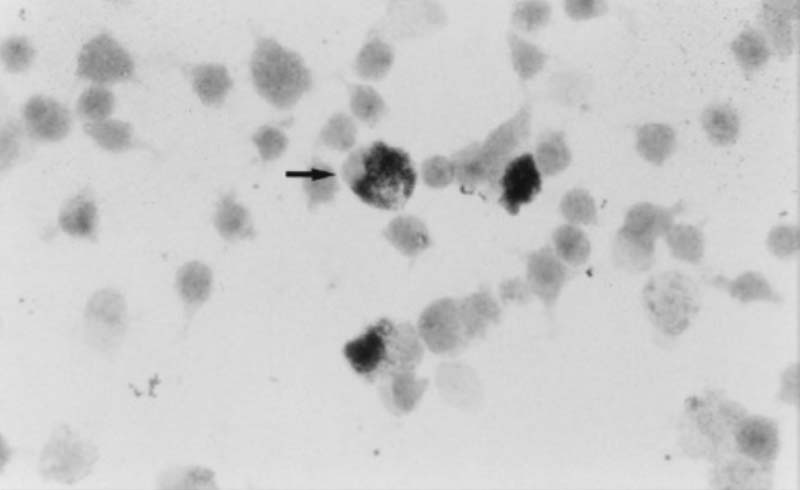
C burnetii is a small gram-negative bacterium and obligate intracellular pathogenic parasite that can infect humans, cattle, goats, sheep and many other mammals (Figure 2). Infection is commonly through inhalation and the bacterium can persist for extended periods of time in the environment – and spread long distances in the wind (Barberio et al, 2017). Climate change may contribute to changing disease patterns (Statham et al, 2017).
The main risk factor for infection is livestock density (Clark and Soares Magalhães, 2018; Hawker et al, 1998). It is thought the disease may also be transmitted by ticks or other arthropods (Maurin and Raoult, 1999).
In humans, infection usually occurs through inhalation of dust or aerosols containing the pathogen shed by ruminants; therefore, an increased risk of disease exists for ruminant vets and farmers.
Pathogenesis
Following inhalation of the bacterium, haematogenous spread and then infection of organs occurs. Severity of disease depends on the immunocompetence of the infected animal or human and other factors.
In farm animals, bacteria tend to localise in the placenta (Barberio et al, 2017). Domestic ruminants (goats, sheep and cattle) are the major reservoirs and sources of human infection (Maurin and Raoult, 1999) – goats are the most susceptible, clinically manifesting with abortion and reproductive problems, followed by sheep and cattle. Infected animals can shed bacteria in significant numbers at parturition; the placenta can have up to 109 bacteria per gram. Bacteria are also shed in milk, faeces and vaginal mucus, milk being the primary route in cattle (Rodolakis et al, 2007).
The timing and degree of shedding can vary significantly and contribute to the environmental contamination.
Prevalence
PCR testing of bulk milk across 155 herds in 2009-2010 in south-west England revealed a 70% prevalence (Valergakis et al, 2012), falling within the 38% to 94% range of herd prevalence previously reported in Europe and North America using bulk tank milk (BTM) or serum samples (Capuano et al, 2001).
Velasova et al (2017) found the prevalence of Salmonella species and C burnetii in a population of dairy herds in Great Britain was approaching 80% (Figure 3).
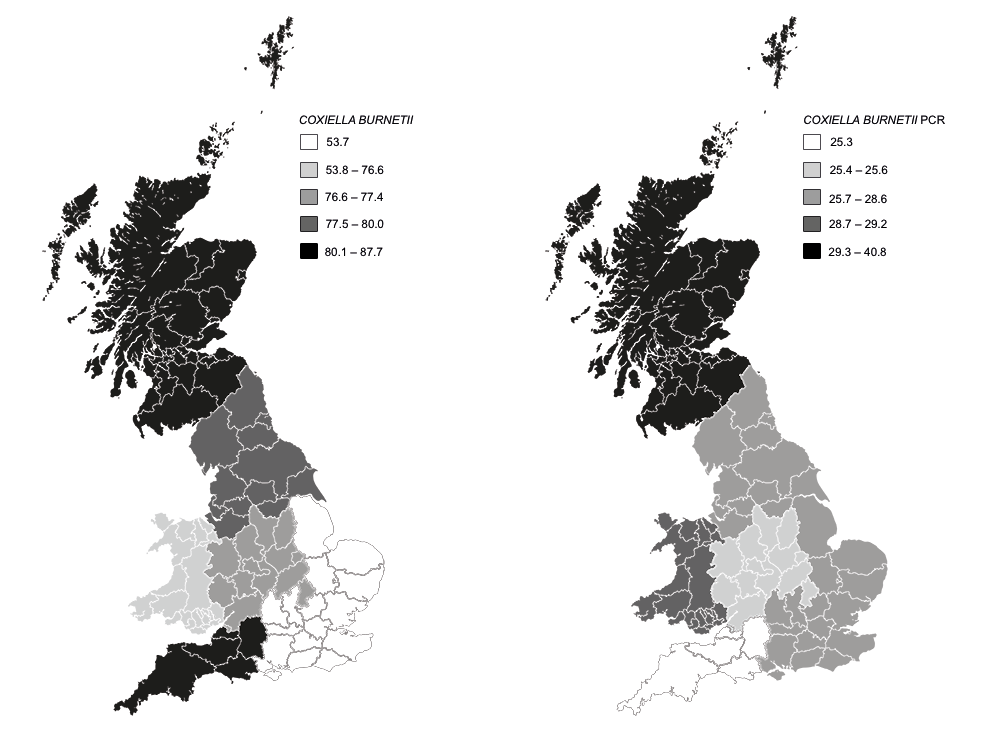
In a survey carried out on bulk milk from dairy farms located in south-west and north-east England by RAFT Solutions (2021, data on file), 31 out of 50 (62%) positive BTMs were recorded overall by PCR, with 14 out of 28 (50%) positive results from south-west England and 18 out of 25 (72%) positive results from north-east England.
Historic infection was completely absent in some herds, but at more than 60% prevalence overall.
Clinical signs
In cattle, clinical signs associated with Q fever infection include:
- Increased risk of abortion, still birth, premature and/or weak calf births (Cabell, 2007; Barberio et al, 2017; Wouda and Dercksen, 2007; Figures 4 and 5).
- Increased risk of retained fetal membranes (RFM; Valla et al, 2014).
- Increased risk of metritis and endometritis (Valla et al, 2014).
- Infertility (Valla et al, 2014; Dobos et al, 2020):
- increased calving to conception intervals
- increased returns to service
- poor pregnancy rate (Valla, 2014; Dobos et al, 2020)


This is, therefore, overwhelmingly a disease with reproductive impacts for cattle. Clearly, these clinical signs are not 100% specific presentations of Q fever, and it is important to carefully consider other potential causes, such as other infectious disease, semen quality or nutrition, and investigate appropriately.
However, a number of studies across several countries are consistent with significant association of Q fever infection with the clinical signs previously mentioned.
In goat herds, clinical signs associated with infection include the following (Van de Brom et al, 2015):
- increased abortion, stillbirth or weak newborn kids
- increased RFM
- milk drop
As with cattle, it is important to rule out other infectious or management causes of losses.
Although Q fever in humans is asymptomatic in 60% of cases, it can lead to acute or chronic infections, and cause flu-like syndrome, hepatitis, pneumonia, endocarditis or abortions.
In Australia, Q fever has long been recognised as an important zoonoses and it is the most commonly notified zoonotic disease.
In the Netherlands, a steep increase in the number of human cases was observed in 2007 to 2009. A link was established between some human cases and farms of small ruminants where abortions due to Q fever were detected.
Diagnosis
Due to the nature of the disease and variation in shedding, diagnosis can be challenging.
Clinical signs are common to other infectious diseases, such as BVDv, leptospirosis and IBR, in addition to nutritional deficiencies or semen quality effects, and so, differential diagnoses should be carefully considered before concluding that Q fever is the causative agent for reproductive performance issues in dairy or beef herds (Statham, 2011a and 2011b; Statham et al, 2019; Cabell, 2007).
It should also be noted that infected animals can be asymptomatic, but still be shedding the bacteria; animals can also shed from differing routes and the amount of shedding can vary significantly over time. In cattle particularly, the presentation is often subclinical and can be confused/diluted by other factors. However, Q fever should be considered when other important causes of reproductive losses are ruled out and clinical signs are consistent with those described previously.
Diagnostic tests for C burnetii should be considered for investigation of reproductive disease. A combination of PCR and serology testing can represent a helpful approach. Without routine screening, infected herds may remain undetected and pose a risk for disease transmission to other ruminants and humans – especially in areas with high cattle density.
Serology
ELISAs measure antibody levels, which can be a useful indicator of exposure to the bacteria in unvaccinated animals, although historic exposure can require careful interpretation. Blood sampling, for example, six problem cows for serology can be a helpful diagnostic tool.
- Select a minimum of six cows with clear recent history of reproductive issues (RFM, metritis and stillbirth, for example) and six bulling heifers.
- If more than 50% is serology positive (and/or BTM PCR positive), then C burnetti is likely to be circulating in the herd and Q fever may well be involved.
PCR
PCR can be run on a variety of biological (for example, bulk milk or cervical fluid), and environmental samples to demonstrate presence of the bacteria. Due to its zoonotic nature, fresh samples can be a risk to laboratory staff. When investigating abortion in cows, PCR can be performed on cervical swabs, ideally on a minimum of two aborted dams, or alternatively on placenta or the aborted fetus (liver, spleen, stomach contents). Sampling must be done within eight days following the abortion and samples should be refrigerated and sent to the lab as soon as possible.
Q test
Recent work has validated the Q test for use on BTM samples from dairy herds and may allow improved detection rates (Treiles et al, 2021).
Reportable disease and The Zoonoses Order
C burnetii (Q fever) was added to The Zoonoses Order in February 2021 in England, and in April 2021 in Wales and Scotland.
What has to be reported:
- All positive PCR results (even if more than one positive from the same farm), including Q test.
- Modified Ziehl-Neelsen smears on placental samples and suspicious of Q fever should be sent for further analysis to the APHA Penrith veterinary investigation centre (sending fresh placenta with cotyledon) to confirm by PCR.
- Serology – if only serology is done, only report to APHA if concerns exist regarding Q fever on the farm. Confirmatory PCR testing will then need to be carried out.
Treatment and prevention
Treatment
Limited efficacy exists in the use of antibiotics (oxytetracycline) in small ruminants and cattle (Ordronneau, 2012; Astobiza et al, 2013). However, with growing awareness of antimicrobial resistance as part of one health, it is increasingly inappropriate to rely on blanket antimicrobial therapy for control in livestock health and welfare, unless other avenues are first fully considered (Taurel et al, 2012).
Prevention
Prevention measures consist of strict biosecurity and environmental hygiene. Infected animals shed large quantities of bacteria into the environment through faeces, vaginal mucus, urine, milk and – especially – parturition products. C burnetii survives very well in the environment, and contaminates aerosols and dust.
Any control measure leading to a decrease in either the prevalence of shedders or in the environmental bacterial load will help limit both the spread of the infection in ruminants and the zoonotic risk. Environmental measures include destruction of placentas and disinfection of birth locations.
Vaccination
Coxevac (Ceva) is a phase-1 inactivated vaccine against C burnetii. Dose is 4ml for cattle and 2ml for goats, given under the skin. The primary course is two injections given three weeks apart. A vaccine protocol needs to be implemented across at least three years to maximally reduce shedding and, therefore, environmental contamination and disease (Figure 6). Ideally, primary vaccination should be completed before first service.

In a study by Courcoul et al (2011), the long-term effectiveness of three different vaccination strategies in a recently infected dairy cattle herd was studied through a modelling approach. The vaccination scenarios tested in the study were:
- vaccination of the whole herd for 10 years
- vaccination of the whole herd for 3 years
- vaccination of the heifers only for 10 years
Scenario one was predicted to be the most effective control strategy. In fact, all three vaccination strategies reduced the prevalence of shedders, the environmental bacterial load and the number of abortions; however, effectiveness was not equivalent.
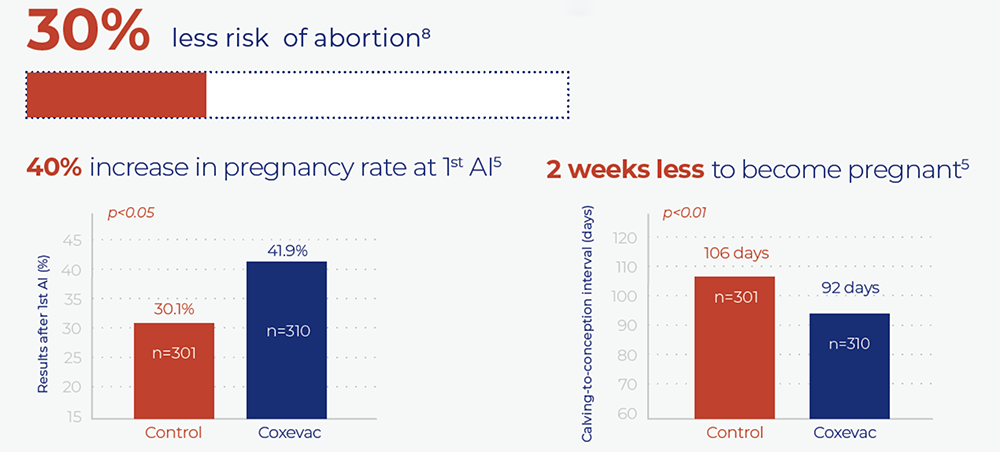
Since the infection was seldom eradicated in the first years of vaccination, an early cessation of vaccination (as in scenario two) could prove ineffective in the long run. Its short-term effect on infection dynamics depends on the duration of immunity for effectively vaccinated cows. Lopez Helguera et al (2014) showed that vaccinating against Q-fever with an inactivated phase-1 vaccine (Coxevac) improved reproductive performance in C burnetii-infected dairy herds (Figure 7).
Conclusions
C burnetii-infection causing Q fever is commonly found in the UK, Europe and internationally, with recent surveys showing seroprevalence ranging circa 60% to 80% in bulk milk in the UK.
Q fever has underestimated consequences. It is a cause of reproductive diseases in cattle and small ruminants, and a zoonosis, but remains a disease with low levels of recognition in the UK.
Although its impact should be considered with appropriate diagnostics and alongside other potential causes, the gap between recorded prevalence and perception is wide.
An 820-cow closed Holstein dairy herd, milking three times per day, had a mean annual production of 10,400kg milk/year at 4.4% fat and 3.5% protein. BVD had been successfully eradicated and good control of major infectious diseases had been established, such as IBR and Neospora, with low risk of Johne’s disease.
Nutritional management was effective, with incidence of ketosis less than 10% in fresh cows and left displaced abomasum incidence less than 1%, and clinical mastitis rate was 12 cases per 100 cows per year, with bulk milk somatic cell count at 90,000 cells. Calving interval was 387 days; however, despite this and excellent reproductive management systems, rates of fetal loss were a concern, with cows’ pregnancy diagnosis (PD) negative after confirmed PD positive. Endometritis rates were 34%, resulting in high levels of topical antimicrobial washout treatments for fresh cows.
Regional surveys of herds using a Q-test as PCR evaluation of bulk milk and cohort serological testing allowed a comparative evaluation of Q fever status, alongside targeted PCR testing of abortus material.
This herd showed a high prevalence in the survey – as in Tables 1 and 2, and interpreted in Figure 8 – with Q-test positive on bulk milk, while abortus material samples, including placenta, were positive for Coxiella burnetii.
| Table 1. Q fever serology results from case study | |||
|---|---|---|---|
| Our ref | Your ref | Sample material | Q fever antibody by ELISA |
| 3222165 | 5556 – C | Serum | 246 |
| 3222166 | 3924 – C | Serum | 112 |
| 3222167 | 4820 – C | Serum | 11 |
| 3222168 | 4870 – C | Serum | 30 |
| 3222169 | 4657 – C | Serum | 173 |
| 3222170 | 7053 – C | Serum | 81 |
| 3222171 | 7385 – H | Serum | <1 |
| 3222172 | 7448 – H | Serum | <1 |
| 3222173 | 7434 – H | Serum | <1 |
| 3222174 | 7443 – H | Serum | <1 |
| 3222175 | 7453 – H | Serum | <1 |
| 3222176 | 7451 – H | Serum | <1 |
| 3222177 | 4864 – C | Serum | 192 |
| Table 2. Q test results | |
|---|---|
| Positive | 37,93 |
This initiated a review of hygiene measures at calving and vaccination programme against Q fever.
References
- Astobiza I et al (2013). Evaluation of the efficacy of oxytetracycline treatment followed by vaccination against Q fever in a highly infected sheep flock, Vet J 196: 81-85.
- Barberio A et al (2017). Epidemiology of Q fever in cattle. In Caetano Simõaes et al (eds), The Principles and Practice of Q Fever: The One Health Paradigm, Nova Science Publishers, New York: 189-212.
- Cabell E (2007). Bovine abortion: aetiology and investigations, In Pract 29(8): 455-463.
- Capuano F et al (2001). Influence of three types of farm management on the seroprevalence of Q fever as assessed by an indirect immunofluorescence assay, Vet Rec 149(22): 669-671.
- Clark NJ and Soares Magalhães RJ (2018). Airborne geographical dispersal of Q fever from livestock holdings to human communities: a systematic review and critical appraisal of evidence, BMC Infect Dis 18(1): 218.
- Courcoul A et al (2011). Modelling effectiveness of herd level vaccination against Q fever in dairy cattle, Vet Res 42(1): 68.
- Dobos A et al (2020). Serological screening for
in the context of early pregnancy loss in dairy cows, Acta Vet Hung 68(3): 305-309. - Hawker JI et al (1998). A large outbreak of Q fever in the West Midlands: windborne spread into a metropolitan area? Commun Dis Public Health 1(3): 180-187.
- Lopez Helguera I et al (2014). Vaccinating against Q-fever with an inactivated phase-I vaccine (Coxevac) improves reproductive performance in Coxiella burnetii-infected dairy herds, Proceedings of XXVIII World Buiatrics Congress, Cairns, Australia: 274-275.
- Maurin M and Raoult D (1999). Q fever, Clin Microbiol Rev 12(4): 518-553.
- Ordronneau S (2012). Impact de la vaccination et de l’antibiothérapie sur l’incidence des troubles de la reproduction et sur la fertilité dans des troupeaux bovins laitiers infectés par Coxiella burnetii, INRA, ONIRIS, 1300 BioEpAR Biologie, Epidémiologie et Analyse du Risque. Centre de Recherche Angers-Nantes, Nantes, France.
- RAFT Solutions (2021). A Survey of Coxiella burnetii exposure in dairy herds in NE and SW England, data on file.
- Rodolakis A et al (2007). Comparison of Coxiella burnetii shedding in milk of dairy bovine, caprine, and ovine herds, J Dairy Sci 90(12): 5,352-5,360.
- Statham JME (2011a). Cattle health schemes, In Pract 33(5): 210-217.
- Statham JME (2011b). Cattle health schemes, In Pract 33(6): 282-285.
- Statham JME et al (2017). Climate change and cattle farming, In Pract 39(1): 10-19.
- Statham JME et al (2019). Looking after the bull, In Pract 41(2): 69-83.
- Taurel A-F et al (2012). Effectiveness of vaccination and antibiotics to control Coxiella burnetii shedding around calving in dairy cows, Vet Microbiol 159(3-4): 432-437.
- Treilles M et al (2021). QTest: a new way to easily sample, store, and ship samples to perform Q Fever PCR analysis on bulk tank milk, JDS Commun 2(6): 409-414.
- Valergakis GE et al (2012). Coxiella burnetii in bulk tank milk of dairy cattle in south-west England, Vet Rec 171(6): 156, 1-2.
- Valla G et al (2014). Prevalenza di Coxiella burnetii nel latte di massa in allevamenti di bovine da latte italiani e possibile correlazione con problemi riproduttivi, Large Anim Rev 20: 51–56.
- Van de Brom R et al (2015). Coxiella burnetii infections in sheep or goats: an opinionated review, Vet Microbiol 181(1-2): 119-129.
- Velasova M et al (2017). Herd-level prevalence of selected endemic infectious diseases of dairy cows in Great Britain, J Dairy Sci 100(11): 9,215-9,233.
- Wouda W and Dercksen DP (2007). Abortion and stillbirth among dairy goats as a consequence of Coxiella burnetii, Tijdsch Diergeneeskd 132(23): 908-911.